Acromegaly
Synonyms in a broader sense
Pituitary giant growth, growth disorder
English: acromegaly, pituitary gigantism
Definition of acromegaly
Under the term Acromegaly one understands an enlargement of the acra (see below) and the internal organs due to increased Growth hormone - Excretion (somatotropin secretion, GH (growth hormone) secretion).
This excessive secretion occurs after the elongation is complete.
Acras are e.g. E.g. nose, lips, tongue, ears, hands, fingers and feet. If this overproduction occurs before puberty, i.e. if the length growth is not yet complete, a giant growth caused by the pituitary gland develops (pituitary gigantism).
Read more about the topic here: Stunted growth
history
The name acromegaly comes from the Greek akron = point and mega = large. The neurologist Pierre Marie from Paris is considered to be the first to describe this clinical picture.
At the end of the 19th century he recognized the enlargement of the acra (see definition) as a clinical picture. However, there are indications that acromegaly was already known to the Egyptians at the time of the pharaohs.
There are images of pharaohs who are depicted with bulging lips, large chins and protruding noses. At the time, these typical anatomical features of acromegaly were considered divine.
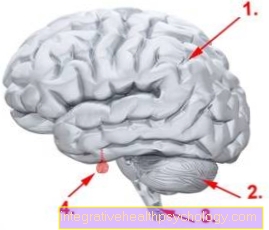
Illustration brain
- Cerebrum (Cerebrum)
- Cerebellum (Cerebellum)
- Spinal cord
- Pituitary gland (pituitary gland)
Frequency / epidemiology
Occurrence in the population
On average, around 40 - 70 people out of 1 million people are affected. Every year around 3 to 4 people per 1 million people get sick.
Cause of acromegaly
As a rule, there is an adenoma (benign tumor) of the anterior pituitary gland (this is a hormone-producing part of the brain), which produces too much of the hormone somatotropin.
An adenoma is a benign tumor that originates from gland cells and tries to imitate them.
In this case it grows in the anterior part of the pituitary gland. In extremely rare cases, the tumor can also be malignant (carcinoma).
The following causes are just as rare: an overproduction of somatotropin, the cause of which lies outside the anterior pituitary gland.
Since the production of this hormone is stimulated by the so-called GHRH (Growth Hormone Releasing Hormone) from the hypothalamus (other brain region), tumor-related overproduction can also occur here in very rare cases.
This increased release would then also lead to an increased release of the hormone somatotropin (Growth hormone) to lead.
Read more on the topic: These symptoms indicate a pituitary tumor!
Symptoms / complaints
Typical symptoms acromegaly are enlargements and coarsening of the skull, the hands and Feet.
This enlargement of the acra is almost always present, as is the Thickening of the skin and a Splanchnomegaly (abnormal enlargement of internal organs).
Acromegaly often occurs in women Menstrual irregularities (Disruption of the monthly period).
In just under half of men there is libido and Erectile dysfunction on. In both sexes there is increased sweating (Hyperhidrosis).
In patients with Acromegaly the protruding eye bulges also fall on the face (prominent supraorbital bulges) on.
The enlargement of the nose, Lips and tongue leads to a typical lumpy language.
Depending on the size of the adenoma it will recur because of its displacing growth a headache and visual disturbances observed.
Also the peripheral Nervous system can be affected: there are sensory disorders (sensory disturbances) in the hands and feet and also muscle weakness.
35-50% of patients will have a Carpal tunnel syndrome with compression of the Median nerve seen.
You can find further information under our topic:
- Carpal tunnel syndrome.
Many patients with existing acromegaly also develop changes in the Cardiovascular system and as a result one high blood pressure.
You can find further information under our topic:
- Cardiovascular system
- high blood pressure
diagnosis
As with any procedure for establishing a diagnosis, the anamnesis (medical history) can provide information:
-
Do old rings still fit, has the shoe size changed?
-
A comparison with old photographs can help.
In endocrinology (the study of hormones) different levels can be measured in the blood:
- IGF 1 in plasma: since IGF 1 is stimulated by somatotropin (STH), it reflects the STH levels
- Basal STH level: a daily profile must be created because STH is released in different concentrations at different times of the day (mostly at night)
- STH values in the TRH and LHRH test: it is tested whether the growth hormone can be stimulated pathologically (i.e. pathologically); The hormones TRH (stimulates the secretion of TSH, which stimulates the thyroid gland) and LHRH (stimulates the secretion of LH and FSH, which in men influence the maturation of the sperm and in women the egg cells) record the function of the anterior pituitary gland (HVL) by measuring the concentration of the affected hormones (TSH, FSH and LH). If the concentration does not rise, then there is an anterior pituitary (HVL) disorder.
Therapy for acromegaly
Is it the root cause around a benign microadenoma (small adenoma) it can be surgically removed.
Approx. 90% of the cases are clinically cured. However, if the adenoma of the pituitary gland is larger than 10mm (macroadenoma = large adenoma), it can also be surgically removed, but it can only be completely removed in about 60% of cases.
The result can be seen immediately after the operation because the IGF 1 level drops. The clinical symptoms, however, only slowly recede over weeks and months.
In patients for whom an operation is not an option or if surgical therapy fails, radiation therapy can help. For this purpose, using CT (computed tomography) or MRI (magnetic resonance tomography) Recordings and, with the help of a computer program, individually tailored radiation plans are created for each patient. These include the strength, location and frequency of the radiation. However, the full effect only occurs after a few years.
Drug therapy can also be used. This is z. E.g. used when an operation or radiation cannot be performed, or in preparation for both.
It will Somatostatin analogs (Substances that correspond to somatostatin and show the same effect: octreotide, lanreotide) and Dopamine agonists (Substance that has the same effect as dopamine; Dwiropamine is the precursor of adrenaline).
The Somatostatin-Analogues lead to a reduction in the STH level in many patients (80-95%).
In half of the patients, the adenoma even shrinks.
As disadvantage the hormone is seen to be injected under the skin and is relatively expensive. However, it is also increasingly being injected into the muscle, where it has a depot effect for 2-4 weeks.
Problems affecting the gastrointestinal tract (e.g. diarrhea) can occur at the beginning of therapy. One advantage, however, is that the effect can be assessed quickly (within hours).
On the Dopamine agonists unfortunately only address about 25% of patients. The dopamine agonist cannot cause the adenoma to shrink either. The effect can be assessed within a few weeks (6-8).
A relative new development is a receptor antagonist, which prevents the effect of the STH at the docking point (receptor) of the hormone. So it does not lead to a direct lowering of the STH concentration. Like the other drugs, it is used when surgical therapy or radiation has either not been effective or is not possible.
forecast
If the benign tumor can be operated on, the likelihood of complete healing depends on its size.
The effective cure rate for microadenomas is 90%, for macroadenomas it is still 60%.