Internal rotation gait in children - is it dangerous?
General
Every person has his own way of walking. “Shuffling”, “waddling” or “walking over the great uncle” are just a few of the colloquial terms for gaits that can make a person stand out.
Most people who hear one of these terms, however, move in the normal range of gait variety despite the variety. The typical gait of small children is also unmistakable when they turn their legs inward (= internal rotation) and walk in the so-called internal rotation walk, colloquially “over the great uncle”.
The toes then typically point towards each other when walking. This makes children look very cute and up to the age of four this is perfectly fine and normal if the child shows normal hip development. This early childhood form of internal rotation in children is completely harmless and usually resolves completely spontaneously and without medical intervention.

My child is showing an internal rotation gait - how dangerous is that?
Only when a healthy child maintains this gait pattern after the fourth year of life is there a need for clarification, because only then is it a clinical picture which can lead to the development of various long-term unfavorable consequential damages that are associated with late-stage damage such as chronic pain and premature joint wear (osteoarthritis) .
Even if children have passed this "magical age threshold", the gait pattern disappears by itself in 90% of children, at the latest when they are fully grown and no treatment is required.
However, if there is an organic cause, such as hip dysplasia, this should be treated accordingly in order to avoid further late damage associated with the clinical picture.
causes
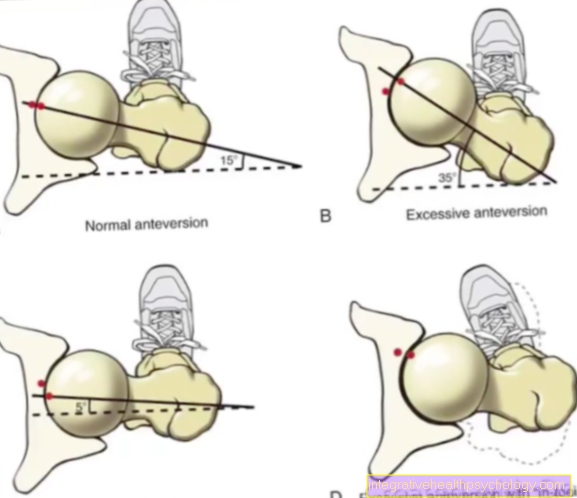
The causes of the internal rotation are varied. The most common reason is one hip socket turned forward (Coxa antetorta). The hip socket (lat: Acetabulum) forms the cavity in the pelvic bone that contains the Femoral head and in which he feels like a Ball joint can move.
The hip joint connects the trunk with the legs. Here takes place by many bone, Muscles and Joints the power transmission takes place and only enables the optimal stability of the gait. Disturbances in this area affect the statics of the entire body.
Is this cavity in the pelvic bone too far now? frontAs is the case with the coxa antetorta (coxa = hip; ante = front), the Position of the entire leg in relation to the body. Fit through the front layer Femoral head and acetabulum no longer optimally to one another as long as the legs are straight and Kneecap and feet are parallel, as is usually the case.
To be flawless as a ball-bearing to function, the child must follow the leg Inside Turn to achieve the optimal position of the femoral head in the pan. Outwardly it comes to Internal rotation gait of the child, visible by pointing the kneecaps and feet towards each other.
Hip dysplasia as the cause

Another cause is the congenital malalignment of the hip joint, the so-called hip dysplasia. Here, the hip sockets are not correctly applied during the child's development and the ball joint cannot be designed in its optimal form.
In the maximum variant, the head of the thigh bone cannot protrude into its counterpart, the acetabulum, and move there, and is even located outside the joint. The infants are noticeable early on because they cannot spread their legs and the folds in the groin look different.
This disorder often occurs in families and can be diagnosed early on with an ultrasound scan and treated with splints. These press the head of the thigh against the pelvis so that a suitable cavity is formed there over time.
This cave is often not formed at the optimal point in the pelvis, and here too the image of the internal rotation path results from the rotation of the entire leg.
Other possible causes

If the hip is not to blame for walking over the great uncle, the leg itself is also a possible “culprit”. The hips and thighs can be completely healthy, but the lower leg can be rotated below the knee joint and even then the children walk in internal rotation.
Fractions (= fractures) can also grow back together twisted and thus force the leg into the rotational position. In this case, the unilateral internal rotation path arises.
Less common causes of the innate internal rotation gait are clubfoot or arches foot.
The child's hips, thighs and lower legs are completely healthy. The cause lies in the deformation of the foot itself.
Therefore, completely different forms of therapy apply here than with the hip-related internal rotation malalignment, which will not be explained in more detail at this point.
Paralysis caused by various brain damage can typically also be associated with the internal rotation gait and is usually treated as part of the very intensive physiotherapy.
consequences
muscle, Tapes and Tendons adapt to this change in the long run and lose their function. The pool can now only poorly stabilized and the power transmission between the trunk and legs can no longer be carried out effectively.
In the long term, this condition persists Pain and often by one early osteoarthritis (= Joint wear) noticeable. The rest of the skeleton also suffers from this condition. The change in the pelvis also changes the pressure and stress of the Spine.
Children develop excessive curvature of the spine in the lower back (Hyperlordosis). This posture of the spine tries to compensate for the changed statics of the pelvis. However, this also leads to consequential damage such as Back pain, early Herniated discs or premature wear of the Vertebral bodies and their joints.
Furthermore, the knee exposed to other loads, as they are now also loaded in different places than usual with a normal leg position. As in the case of the spine and the hip joint, early wear and tear due to incorrect loading can be the result (=Osteoarthritis of the knee).
therapy
Therapy of the internal rotation gait that persists beyond puberty saves many people from later problems such as pain, osteoarthritis and possibly a hip replacement.
Any consequences for the knees and spine and the rest of the skeletal system can also be prevented by simple means. Only in very rare extreme cases may an operation be necessary.
During this operation, the thigh is broken and fixed again in a rotated normal parallel leg position and the hip joint itself is left in its position.
Torqheel heels
Once the diagnosis of the internal rotation gait requiring treatment has been made, physiotherapy on the one hand and the use of special heels, so-called Torqheel heels on the other, can bring healing.
These special heels are positioned under the child's heel, either in the shoe or under the sole. This corrects the leg axis and straightens the inwardly turned position. Already after six months of treatment great successes can be achieved or the gait pattern can be completely normalized.
physical therapy
Physiotherapy is also a useful therapy method.
The indication for physiotherapeutic treatment should always be made individually depending on the cause of the internal rotation gait. Physiotherapy is especially important in combination with Torqheel heels if the cause of the malalignment is, for example, a coxa antetorta (= hip socket turned forward).
If hip dysplasia is the reason for an internal rotation walk, physiotherapy can be helpful as an accompanying measure to orthopedic aids such as braces.
In severe cases, surgical treatment of an internal rotation duct may be necessary. Then physiotherapy is an integral part of the postoperative therapy scheme.
Overall, the importance of physiotherapy in the therapy of internal rotation in children is high.
Insoles - a sensible therapy for the child's internal rotation walk?
Insoles are not provided in the treatment of the internal rotation path. Since the internal rotation gait in children is an error in the gait pattern with a very high rate of spontaneous correction, therapy should generally be cautious at first. It is not uncommon for the internal rotation path to recede in children after puberty.
Even if this is not the case, wearing orthopedic measures such as an insert makes little sense. This is because the cause is usually an incorrect position of the hip joint, more precisely an enlarged femoral neck angle. If the leg position were corrected, the femoral head would not be adequately encompassed by the acetabulum. This can lead to further complaints, so that children have not been helped by wearing insoles during internal rotation.
However, a Pomarino insert, a corrective rotation insert, makes sense. However, this is not a conventional insert. It is a modified form of the Torqheel heels: The heels are then not attached under the shoe as they should be, but processed in the insole in the shoe.



.jpg)