Artificial coma when you have pneumonia
introduction
Severe pneumonia can lead to lung failure if the outcome is unfavorable. Those affected are then usually connected to ventilators or lung replacement devices and put into an artificial coma.
In contrast to a coma, sleep is artificially generated by medication and is then monitored and controlled by specially trained doctors, so-called intensive care physicians.

Why do you need an artificial coma with pneumonia?
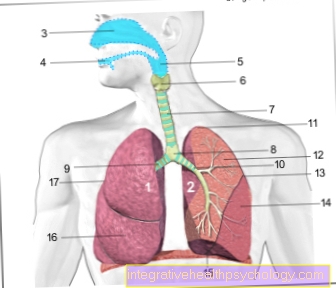
The artificial coma in pneumonia is used when the lungs no longer function properly - in medical jargon, lung failure is then spoken of (see also: Acute respiratory failure). If conventional therapeutic measures for treating pneumonia are no longer sufficient, those affected are usually dependent on mechanical ventilation / oxygen supply.
This can be done using a ventilator, in which a tube is placed in the airways, or a lung replacement device or procedure. In the lung replacement procedure, the oxygen is then transported into the body through an access into the blood vessels; the lungs are then no longer involved in the oxygen exchange process.
This special device is also known as ECMO (extracorporeal lung membrane oxygenation). In order to use the “lung function devices”, those affected are then put into an artificial coma. The artificial coma makes it possible to tolerate a ventilation tube in the oral cavity or the airways and also helps to protect the body, in particular from stress and pain.
This protective mechanism is achieved through the anesthesia, or through the medication, which on the one hand “let the patient sleep” and also has a pain-relieving effect. The artificial coma for pneumonia is not a standard procedure, but is only used in extreme cases, especially when all other therapeutic measures have shown no effect and there is a loss of lung function.
Find out more about the topic here: The therapy of pneumonia.
Duration of the artificial coma in pneumonia
A general statement about the duration of the artificial coma in pneumonia cannot be made. The artificial coma is primarily used to relieve the body or to stabilize the circulation, which are endangered by pain and stress.
The necessary length of time for an artificial coma depends on the patient's progression values and is then assessed by specialist doctors, usually anesthetists. In general, an attempt is made to keep the artificial coma as short as necessary, since maintaining the artificial "sleep" for a very long time increases the risk of complications.
Tracheal incision
In a tracheal incision, the trachea is opened in the neck through a small operation, thus creating access to the airways and the associated lungs. Such an operation is also called a tracheal incision (Tracheotomy, lat.trachea = Windpipe) called.
A tracheal incision is used, among other things, for long-term ventilation. The ventilation tube then does not have to be inserted through the mouth, but can be placed directly through the interface in the windpipe and thus ensure an adequate supply of oxygen to the affected person.
In the case of severe pneumonia and an artificial coma, long-term mechanical ventilation with an incision in the trachea can be used to maintain the oxygen supply.
For further, more detailed information on this topic, the editors recommend the article: Tracheal cut
forecast
A prognosis depends on various factors. In addition to pneumonia, age and other diseases also play a role. It is therefore not possible to make a general forecast. In this context, only the attending physician can make a statement about the course of the disease or the outcome.
Taking into account the above-mentioned factors in conjunction with the current values of blood and vital parameters or circulatory parameters, this can then make a statement about the course of the disease and the associated prognosis of the person concerned.
Generally speaking, a long period of stay in an artificial coma is associated with a worse prognosis than short treatment.
How quickly does the patient wake up again?
The artificial coma is a "sleep" that is induced by drugs - it could also be called artificial sleep. In addition to sleep-inducing drugs, pain killers are usually also administered. The duration of sleep is related to the medication administration.
If sleep is to be interrupted or ended, discontinuation or dose reduction is necessary. This is carried out by special specialists, so-called intensive care physicians. How quickly a patient wakes up depends on the previously given dose of sleep aid, in medical terminology Narcotics called, and can be actively controlled by the attending physician.
Long term consequences
The long-term consequences of an artificial coma associated with pneumonia are difficult to predict. Ending the artificial coma can lead to various, mostly temporary complaints for those affected. These include: drowsiness, memory lapses and impaired perception.
Delirium, colloquially also passage syndrome, can also occur. This is characterized by sleep disorders, circulatory problems, hallucinations and forgetfulness. Mostly these are side effects that will resolve over time or be treated with certain medications.
The long-term consequences usually result from the underlying disease or the circumstances that led to the use of an artificial coma. If pneumonia requires an artificial coma, it can be assumed that the lungs have almost lost their function.
The use of lung function devices such as the ECMO can take over the lung function for some time by enriching the blood outside the body with oxygen using a special device and then transporting it back into the body's circulation.
In the long term, however, if the lung function is completely lost, it may be necessary to carry out a lung transplant in order to ensure that the body is supplied with oxygen again, since the lung replacement procedure can also be associated with long-term complications or additional stress on the body.
The symptoms of pneumonia are not always limited to the lungs, but can cause other serious symptoms by spreading bacteria into the bloodstream. Read also: Consequences of pneumonia
Additional informationYou can find more information on the topic of "Artificial coma in pneumonia" at:
- Acute respiratory failure
- ECMO
- Tracheal incision
- Continuity syndrome
- Lung transplant