Cauda equina syndrome - do I have paraplegia?
Definition - what is cauda equina syndrome?
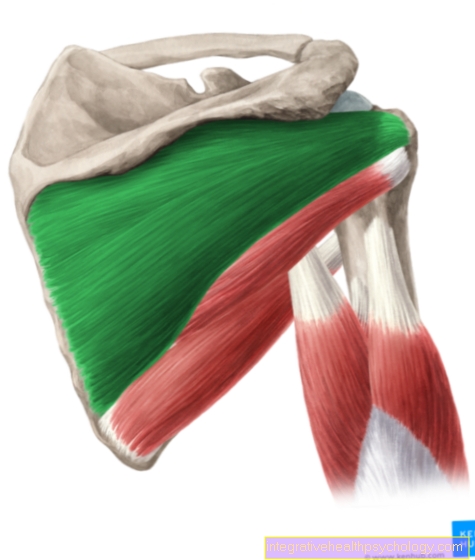
The cauda equina syndrome, or the cauda equina compression syndrome, describes a clinical picture that is characterized by various neurological deficits. As the name of the disease suggests, it is based on damage to the lower spinal cord, the so-called cauda equina. This part of the spinal cord no longer consists of actual nerve cells like the upper part, but represents a collection of nerve roots (spinal nerve roots). It is located below the fifth lumbar vertebra. If this section of the spinal cord is damaged, various neurological deficits result depending on the extent of the damage. These include paralysis of the lower legs, bladder and anus muscles, the failure of reflexes, sensory disorders and many more. Such damage can be caused by herniated discs, tumors or traumatic events.

Causes of cauda equina syndrome
There are many different causes that can lead to damage to the lower spinal cord, the cauda equina. Most causes initially lead to a constriction of the spinal cord due to external compression. This constriction then leads to increased pressure on the spinal nerves running here, which can then no longer perform their function.
The most common causes of cauda equina syndrome include degenerative changes in the spine, such as osteoarthritis. Pronounced osteoarthritis can lead to osseous remodeling processes, which are associated with the formation of smaller bone processes, so-called osteophytes. These can press on the spinal cord and cause symptoms such as paralysis of the lower legs, the bladder and anus muscles, the failure of reflexes, and sensory disorders. However, bone loss (osteoporosis) can also lead to this clinical picture due to the reduced bone density and the associated high risk of vertebral body fractures. Non-degenerative causes such as herniated discs or acute trauma can also be causes of cauda equina syndrome. Another possible cause is the so-called spondylolisthesis, in which neighboring vertebral bodies shift against each other and thus lead to a narrowing of the spinal cord. In addition to this mechanical damage to the spinal cord, inflammatory processes in the area of the cauda equina can also lead to a loss of function of the spinal nerves. Other possible causes are ankylosing spondylitis, metabolic changes, tumors and diseases of the blood vessels.
The complete cauda equina syndrome
A complete cauda equina syndrome is when the entire lower spinal cord is compressed in the area of the cauda equina and the spinal nerves show a complete loss of function. Thus, the entire cauda equina syndrome can be assigned to the so-called paraplegic syndromes. Since all spinal nerves running here are compressed, the entire spectrum of symptoms that is typical for cauda equina syndrome usually occurs. These include paralysis of the lower leg, foot and toe flexors and the gluteal muscles, incontinence due to paralysis of the bladder and anus muscles, failures of reflexes, as well as sensory disorders on the inner thighs, as well as the back of the legs and the outer edge of the foot. Complete cauda equina syndrome is an acute neurological emergency and should be treated for neurosurgical treatment as quickly as possible, as the risk of irreversible damage increases significantly over time.
The incomplete cauda equina syndrome
With incomplete cauda equina syndrome, only parts of the spinal nerve bundle are compressed. So there is no complete loss of functionality here. In the case of incomplete cauda equina syndrome, the exact severity of the symptoms depends on the exact location of the compression on the spinal cord. Thus, for example, symptoms of paralysis can only occur on one half of the body, whereas the other side is not affected. Furthermore, it is possible to only be able to detect failures in motor skills or loss of sensitivity without a functional restriction of urinary and stool continence being recognized.
Symptoms of cauda equina syndrome
The complete cauda equina syndrome is accompanied by paralysis of the lower leg, foot, flexor toe and gluteal muscles with other, sometimes very stressful, symptoms. Since the continence of the bladder and rectum is controlled by spinal nerves that are below L5, a cauda equina syndrome usually results in temporary incontinence, which can be irreversible depending on the duration up to the start of therapy. Furthermore, cauda equina syndrome is often associated with severe pain for those affected, which is caused by compression of the spinal nerves. Another symptom of the complete cauda equina syndrome is loss of sensitivity in the area of the inside of the legs, the perineal region and the back of the legs. In addition, erectile dysfunction can occur in men.
Urinary retention in cauda equina syndrome
The term urinary retention means that the urinary bladder can no longer fulfill its function of excreting urine and that the urine accumulates in it. The consequence of cauda equina syndrome is the so-called flaccid bladder. The muscles of the urinary bladder wall no longer receive any information through the spinal cord and thus remain limp. Reflexes are also no longer present. Since the muscles of the urinary bladder now receive no information to tense up and thus empty the urinary bladder, the urine collects in the bladder. In addition to recurring urinary tract infections, this process can lead to increasing damage to the kidneys due to the urine build-up. To counteract this process, what is known as intermittent self-catheterization is used. Those affected can insert a catheter into their bladder themselves and thus empty it.
You might also be interested in: How is urinary retention treated?
Incontinence in cauda equina syndrome
In addition to the case of urinary retention described above, cauda equina syndrome can also lead to urinary and fecal incontinence. The former often represents what is known as overflow incontinence, which occurs when the urinary bladder is felt so strongly with urine and the pressure is too high. The result is unwanted urine excretion. In fecal incontinence, the relaxation of the external sphincter is particularly important, which means that defecation can no longer be controlled voluntarily.
More about this topic can be found: Incontinence
Bladder and rectum disorder in cauda equina syndrome
The term bladder and rectum disorder describes a spectrum of symptoms that, in addition to urinary and fecal incontinence, includes sensory disorders in the genital and anal area and a residual urine sensation. This disorder represents a neurological emergency and requires immediate clarification and treatment in order to prevent irreversible consequential damage. The most common cause of bladder and rectal disorder is cauda equina syndrome.
Treatment of cauda equina syndrome
Cauda equina syndrome is a neurosurgical emergency that needs to be treated immediately. Conservative therapy should not be sought if symptoms such as paralysis are present. The aim is to remove the compression of this section of the spinal cord as quickly as possible in order to prevent irreversible consequential damage such as incontinence. There are many different methods to achieve this goal today, ranging from larger open surgeries to minimally invasive techniques. Which surgical method is used depends on the one hand on the underlying cause, but also on the compression pattern and the surgeon's experience.
Duration of cauda equina syndrome
The length of time the symptoms of cauda equina syndrome persist depends largely on when the therapy was started. If cauda equina syndrome is diagnosed, neurosurgical intervention should be performed within the next 24-48 hours. Any further delay increases the risk of irreversible damage to the spinal nerves, which can be associated with permanent paralysis, incontinence and sensory disorders. Only in very rare cases can the spinal nerves recover from prolonged constriction.
The prognosis for cauda equina syndrome
The decisive factor for the prognosis of cauda equina syndrome is, on the one hand, the time between the onset of symptoms and adequate therapy. But the basic compression pattern and the associated symptoms also have a great influence on the prognosis of the individual patient. For example, an external sphincter weakness or urological symptoms are associated with a poorer prognosis of regaining full function after the operation.
How is cauda equina syndrome diagnosed?
The diagnosis of cauda equina syndrome is a combination of a good clinical-neurological examination and various imaging measures.The clinical examination usually begins with various functional tests that check for possible paralysis of the leg and gluteal muscles. This includes, for example, the one-legged stance, the toe stance, and lifting the leg against a wind stance. The next step is to test the various reflexes, such as the hamstring reflex. This is followed by checking the sensitivity in the area of the legs. If there is already a suspicion of cauda equina syndrome, the clinical examination is extended to the perineal region and the sensitivity, the anal reflex and the sphincter muscle strength are checked here. If, after this examination, there is a suspicion of cauda equina syndrome, an imaging procedure, usually an MRI, is carried out as quickly as possible to show the narrowing of the spinal cord. In most cases, this can be used to secure the suspected diagnosis.
MRI for suspected cauda equina syndrome
An MRI of the lumbar spine is an indispensable part of the diagnosis of cauda equina syndrome. This imaging procedure can also show small constrictions in the spinal cord and determine their extent. Furthermore, it is often possible to determine the exact cause of the compression. In this way, herniated discs, vertebral body fractures, tumors or other causes of cauda equina syndrome can be clearly distinguished from one another.
Checking the anal reflex
The anal reflex describes a contraction of the external sphincter that is triggered by touching the skin on the anus. Thus, the anal reflex is considered to be an external reflex, since the sensitive and the executive organ are different. The anal reflex is triggered by the spinal cord segment S3-S5. A lack of this reflex thus indicates a spinal cord problem that is S3 or higher. Since the cauda equina syndrome, by definition, affects the spinal cord sections that are lower than the fifth lumbar vertebrae, this clinical picture also leads to a failure of the anal reflex.