Meniscal tear
Synonyms in the broader sense
Meniscus lesion, meniscus tear, meniscus rupture, meniscus damage
English: meniscus tear

Definition of meniscal tear
A Meniscus lesion (Meniscus tear) represents an injury to one of the two cartilage discs (Menisci), which are located between the thigh and shinbones.
Looking at the bone structure of Thigh and Shin, you can see that they are asymmetrical to each other (round thigh and straight lower leg) and their joint surfaces do not fit together. The meniscus compensates for this asymmetry.
The meniscus consists of two disks of fiber cartilage, the Medial meniscus and the External meniscuswhich you can also see in the picture below.
The menisci serve as a kind of "buffer“, Because they enable an even pressure load, an even transmission of force and help that Knee joint to stabilize.
Illustration of a meniscus tear

Meniscal tear
(= Meniscus rupture)
I - longitudinal tear
II - oblique view (rag tear)
III - radial crack (transverse crack)
IV - basket handle tear (special form)
V - degeneration (wear and tear)
- Inner meniscus -
Meniscus medialis - Outer meniscus -
Lateral meniscus - Posterior cruciate ligament -
Lig. Cruciatum posterius - Anterior cruciate ligament -
Lig. Cruciatum anterius - Femur -
Femur - Kneecap - patella
- Shin - Tibia
You can find an overview of all Dr-Gumpert images at: medical illustrations
Appointment with a knee specialist?
I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Causes of a meniscus tear
Reasons for the meniscus tear range from traumatic (= accident-related) to degenerative (= due to excessive stress). The percentage distribution of the meniscal tear in the area of the meniscus lesions can be described roughly as follows:
- 50% the meniscus lesions are degenerative in nature. This form of meniscus tear occurs in the course of life through increased stress, whereby various occupational groups such as professional footballers, tilers, miners, gardeners, etc., i.e. people who predominantly kneel at work, are affected.
- 40% of the meniscus lesions arise as a result of indirect violence (= secondary traumatic crack formation). Indirect violence includes sudden hyperextension or flexion of the joint, which inadvertently pinches the meniscus posterior horns. Is then on the jammed meniscus Force, for example in the form of a rotation of the lower leg, can be exerted meniscus tear or tear.
- 8% of the meniscus lesions are caused by direct violence (= primarily traumatic meniscus tears), for example through traumatic events in the form of broken bones.
- 2% of the meniscus lesions occur genetically. There are people with genetically determined malformations of the meniscus. The so-called is an example of this Disc meniscus. Cyst formations and increased calcium deposits in the area of the menisci (= Chondocalcinosis) can lead to meniscus tear in the course of the disease.
Symptoms
Patients with meniscus lesions have pain in the area of the knee joint and can often only move the knee joint to a limited extent. The different causes of a meniscus tear provide different pain symptoms:
Traumatic mensicus lesions (accident-related) are usually perceived as very painful, while lesions due to degenerative changes are often difficult to determine even during an examination. Often there are twists in the knee that lead to an injury to the menisci. For more information, read also: Twisted knees - What to watch out for
Various examination methods of the treating orthopedic surgeon in the case of a meniscus tear help to make the diagnosis, but also to exclude other diseases from a differential diagnosis (see: diagnosis)
Read more on the topic: Symptoms of a tear in the meniscus
Signs of a tear in the meniscus
The main symptom of a meniscus tear is severe pain in the affected knee.
The nature of the pain that occurs is basically determined by the underlying disease. An acute meniscus tear, which occurs, for example, as a result of a sports injury, manifests itself in suddenly occurring, severe pain. Chronic cartilage wear, which is associated with a meniscus tear, shows itself as a gradual worsening of the pain.
As a general rule, the pain usually occurs particularly during exercise. In the course of the disease, the pain can also occur when standing or sitting for long periods of time. The signs of a meniscus tear are usually triggered by cartilage fragments, which are located in the joint space and cause the typical pain there.
Find out more about: Acute knee pain - that may be behind it
Diagnosis of a tear in the meniscus
As part of the manual examination at the Meniscal tear the doctor checks the so-called "special Meniscus mark“By so-called Meniscus tests.
To do this, he uses proven standard tests, e.g. Standard tests according to:
- Steinmann
- Apley - Grinding
- Boehler
- McMurray
and - Payr
Here, attempts are made in different ways, for example in the stretched, bent and twisted position, to press the thigh and lower leg joint surfaces together. In the context of the examination methods, injuries to the external meniscus can be distinguished from injuries to the internal meniscus.
Various meniscus tests also provide information about the location of the tear. The Payr standard test indicates an injury in the posterior horn area of the medial meniscus when pain occurs.
Every diagnosis one Meniscus damage begins with the manual examination described above by the doctor. To make this diagnosis of the Meniscus damage To confirm this, other diagnostic methods are also used.
Meniscal tear types

As already mentioned in the context of the forms of therapy, there are different forms of a meniscus tear. Depending on the location of the injury in the meniscus tissue, the following types of tear can be distinguished in the area of the inner and outer meniscus:
- Bucket handle tear (= longitudinal meniscus tear with displacement of torn meniscus parts into the joint)
- Transverse crack (from the free edge to the base)
- Flap tear in the rear or front horn (= a combination of longitudinal and transverse tear)
- Horizontal tear (tear in the longitudinal direction, whereby an upper and lower lip is formed)
- Demolition of the base of the meniscus
The doctor can use various examination methods, usually manual examinations, which also include x-ray diagnostics, to examine the form of the meniscus tear.
Magnetic resonance imaging (MRI of the knee joint)

Here you will find detailed, generally general information with regard to the MRI: MRI
At this point, it should only be pointed out that the MRI can diagnose over 95% of meniscus tears.
Unfortunately, some meniscus tears cannot be seen on the MRI or the tears are worse on the arthroscopy than would be expected on the MRI. Due to the constant improvement in MRI technology, the error rate in MRI in meniscus tears has decreased significantly.
In the case of a meniscus tear, an MRI of the knee joint is the imaging method of choice, as it can depict the cartilage tissue with the greatest accuracy. This is the best way to assess the cracks, their location, shape and extent.
Based on the findings, the optimal therapy for the patient can then be determined. In addition, the MRI examination enables the simultaneous detection of accompanying injuries to the knee joint (cartilage damage, cruciate ligament tear, outer or inner ligament tear).
It is not uncommon for a meniscus tear to damage other structures of the joint, for example the cruciate ligaments, the outer or inner ligaments or the joint capsule.
When the inner meniscus is injured, the inner ligament and the anterior cruciate ligament are sometimes injured at the same time.
This constellation is also known as the "unhappy triad". The entire joint can be examined through the MRI examination and a complete injury report can be made. This is the basis on which the individual therapy to be selected for the patient is justified.
Read more information on this topic at:
- MRI for a meniscus tear
- MRI of the knee joint
X-ray examination
While the X-ray examination is normal for fresh meniscus injuries and therefore hardly provides any information in the context of traumatic damage, it is very meaningful in the case of chronic damage (e.g. permanent occupational stress on the meniscus). Bony changes become visible. An X-ray examination is carried out in at least two different planes so that any accompanying bone injuries can also be excluded.
Sonography (ultrasound examination)
Although the Ultrasound examination is not routinely used, as other forms of examination are more informative, sonography provides information about accompanying ligament injuries.
Especially swelling, Water in the knee and hematomas / bruises can also be shown well with the ultrascahll examination.
Arthroscopy of the knee
To ensure a diagnosis, a Arthroscopy, so one Reflection of the knee joint be performed. While the doctor can diagnose the interior of the joint with greater precision here, the great advantage of arthroscopy is that, under certain circumstances, surgical treatment can be carried out immediately.
Due to the good image quality of the MRI in the case of a meniscus tear, arthroscopy of the knee joint is practically not performed today for diagnostic reasons.
In the "keyhole surgery" the knee is only opened through a small incision in the skin. A rod that takes pictures from the Joint interior to a screen in the operating room, is made through this small incision in the knee joint. Another small incision allows the introduction of a tactile hook, which the texture of cartilage, Cruciate ligament and Menisci tests. The introduction of further instruments via this second incision is then conceivable, so that for example exposed meniscus parts can also be removed directly.
In cases that require surgical treatment (through a knee arthroscopy), additional examinations such as EKG and or Laboratory control of blood values necessary.
Test (s) for a meniscus tear
Various tests are used to diagnose a meniscus tear and assess the location and extent of the injury.
In a physical examination, the knee joint is moved in different ways and the patient's reaction is analyzed. A number of different tests are known for analyzing an injury to the meniscus.
Even slight pain when performing the test is enough to assess the type of injury. There is therefore no need to be afraid of causing great pain. The tests can be used to assess the injury to the menisci and should not be used as a substitute for diagnostic imaging. We always come to make a clear diagnosis and assess the extent of the injury imaging diagnostic methods (please refer: MRI for a meniscus tear) and possibly a Artoscopy of the knee joint for use.
The tests
The so-called Steinmann test must be in a Steinmann sign I. and a Steinmann sign II be divided.
With the Steinmann sign I the knee joint is rotated slightly inwards or outwards by turning the foot. Depending on which rotation occurs pain, the probability is one Medial meniscus tear or External meniscus tear given.
The Steinmann sign II includes a tapping pain test of the joint with the knee extended and bent. Depending on the point at which a headache can be triggered, the respective meniscus is likely to be injured.
The so-called Apley grinding test is performed in the prone position. The leg is bent and rotated inwards and outwards once while the examiner exerts pressure. Depending on the occurrence of the pain, the attending physician can make a statement about the presumably damaged meniscus.
Also the Böhler test allows an assessment of the location of the injury. The lower leg is moved inwards and outwards while simultaneously extending the knee joint.
During the McMurray tests the attending physician feels the gap in the knee with one hand and slowly extends the leg with the other hand. An injury to the respective meniscus can be assessed by perceiving certain movements in the knee joint and the occurrence of special noises.
To assess damage to the inner meniscus, the so-called Payr test for use. The affected person sits cross-legged while the doctor applies pressure on the knee joint from above. If pain occurs here, there is a likelihood of damage to the medial meniscus.
Therapy for a meniscus tear
Indication for surgery
Not every form of meniscus disease requires surgical treatment. For this reason, diagnostics in the context of meniscus diseases, including various diagnostic tests, play a major role.
The location of the meniscus tear is also of crucial importance with regard to therapy. If the lesion is in the area of the outer zone, for example, it can be treated conservatively, for example in the form of a splint and decongestant medication, possibly in combination with punctures and injections.
However, if the doctor finds a massive rupture or a so-called "basket handle" (= longitudinal meniscus tear), the removal of the torn off part of the Meniscus necessary. The torn off part otherwise affects the joint like a foreign body, which will also damage the cartilage in a special way and early on the clinical picture of the arthrosis will effect.
Cracks in the area of the capsule border can be treated with menicoplexy if necessary. This menicoplexy can be thought of as a "Tackle" or a "Sewing on" imagine. However, since the fiber cartilage is only poorly supplied with blood and therefore has only a few metabolic reserves, damage to the meniscus can rarely "heal".
In the meantime, almost all operations in the area of the meniscus are performed arthroscopically. A arthroscopic meniscus surgery is much gentler, helps avoid consequential damage and preserves as much meniscus tissue as possible with maximum utilization of surgical care. In addition, the Duration of arthroscopy on the knee significantly shorter than open knee surgery.
In principle, however, the following principle applies:
"A meniscus tear should be repaired as early as possible to prevent consequential damage."
In order to ensure long-term optimal care of the knee joint is a dynamic Treadmill analysis recommendable. You are welcome to make an appointment in our practice in Frankfurt am Main.
Appointment with a knee specialist?
I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Bandage for a meniscus tear
Next to a number more conservative and surgical measures, which can be used depending on the type of cartilage damage, certain bandages are available to alleviate the symptoms of a meniscus tear.
In general, however, bandages cannot heal the injury and only achieve limited symptom improvement. Treatment by wearing a bandage alone is not recommended. However, this can be useful, for example, in the period up to the planned operation or as additional pain therapy.
The function of the bandages, which can be worn in the event of a meniscus tear, consists in compressing the knee joint. This compression is intended to build up pressure in the joint capsule and thus relieve the meniscus. Depending on the injury and the type of meniscus tear, a bandage works more or less well. If there are foreign bodies in the joint space, an increase in pressure can only achieve limited success, whereas an increase in pressure with simultaneous osteoarthritis achieves good results in symptom control. Whether a bandage proves to be useful in an individual case should be discussed with the attending physician.
Exercise for a meniscus tear
Exercise can be related to a meniscus tear in different ways.
On the one hand, the injury can be caused by certain sports and thus be an expression of a sports injury. On the other hand, for many people who have had a meniscus tear, the question arises as to when physical activity can be recommended again.
The individual Duration of healing after a meniscus tear can vary greatly depending on the type and location of the injury and the therapy chosen.
A recommendation, from which moment on which sport makes sense, should always be given individually.
Depending on how quickly the cartilage heals, exercise can usually be recommended again after a few weeks. Generally speaking, at the beginning knee-friendly sports how swimming or cycling are better than running, which can only be recommended much later.
It is also crucial whether a chronic Cartilage damage in the knee exists or the meniscus tear is caused by an injury.
Injury-related cartilage damage usually occurs in younger, sporty people, and the healing time is correspondingly shorter than with a meniscus tear, which occurs due to osteoarthritis of the knee.
The type of therapy chosen has a major influence on the point at which the knee can and should be partially or fully loaded again.
After a partial removal of the cartilage, the load is usually possible again shortly after the operation, while the knee after a Cartilage transplant should be treated and conserved significantly longer.
Special exercises during the follow-up treatment can be useful and should be carried out according to the recommendations of the doctor and physiotherapist.
A general ban on sport cannot therefore be pronounced, since such a lack of exercise tends to damage the healing process and the mobility in the knee joint.
In addition to the question of when the knee can be loaded again, depending on the prevailing disease, adjustments to the type of sport carried out should be made if necessary.
Sports that are generally associated with very high stress on the knee should be avoided if possible even after the therapy has been successful. This is especially true for those affected who have a Osteoarthritis of the knee suffer because the strain can also destroy existing cartilage tissue and cause further complaints.
Anatomy of the menisci

Excursus meniscus
The meniscus consists of two crescent-shaped fiber cartilage discs, which are positioned between the thigh and lower leg in order, as mentioned above, to prevent the incongruence (inequality) to equalize the articulating bones and thus to transfer shocks evenly to the cartilage of the lower leg. In addition, the meniscus distributes the synovial fluid, which is particularly responsible for protecting the cartilage tissue, as it causes cartilage discs to slide over one another without friction. It also supplies the cartilage tissue with nutrients and is responsible for removing waste materials from the joint space.
The diagram on the right shows the anatomical structure of both menisci.
In the middle, the two menisci are separated by the cruciate ligaments, to the left of the cruciate ligament is the outer meniscus (light blue color), to the right of the cruciate ligaments is the medial meniscus (greyish color). and the posterior cruciate ligament. As you can easily see from the diagram, the volume of the outer meniscus is significantly larger than the volume of the inner meniscus.
Illustration of the menisci

- Inner meniscus -
Meniscus medialis - Inner articular knot
(Shinb.) -
Medial condyle - Transverse ligament of the knee joint -
Lig. Transversum genus - Kneecap ligament -
Ligamentum patellae - Bursa - Bursa
- Outer meniscus -
Lateral meniscus - Outer joint nodules
(Shinb.) -
Lateral condyle - Anterior cruciate ligament -
Lig. Cruciatum anterius - Posterior cruciate ligament -
Ligamentum cruciatum posterius - Femur - Femur
- Shin - Tibia
- Kneecap - patella
You can find an overview of all Dr-Gumpert images at: medical illustrations
At this point, the structure of the meniscus should be described in more detail in order to be able to better understand the function and possible impairments due to injuries in the area of the meniscus beyond the description of the fixation: Both the inner and outer meniscus consists of three parts. The front portion is called
- Front horn (1) called
- the middle part as pars intermedia (2)
- and the rear part as the rear horn (3).
The two menisci are as C- or crescent-shaped structures between Femoral condyles (= Thigh joint rollers) and the tibial head joint surface (lower leg sliding surface). They are fixed by the joint capsule within the framework of adhesions and supplied via their vessels.
It is noticeable that the inner meniscus is connected to the capsule over almost its entire length. This knowledge explains the fact that an inner meniscus is much more immobile than the more strongly curved outer meniscus.
In addition to the outer wall adhesions, both the inner and outer meniscus are also fixed at the end points. These endpoints of a meniscus are called anterior or posterior horn, depending on the position. Both "horns" have numerous sensitive / sensory nerve endings on. Fiber connections also exist between the medial meniscus and the medial collateral ligament.
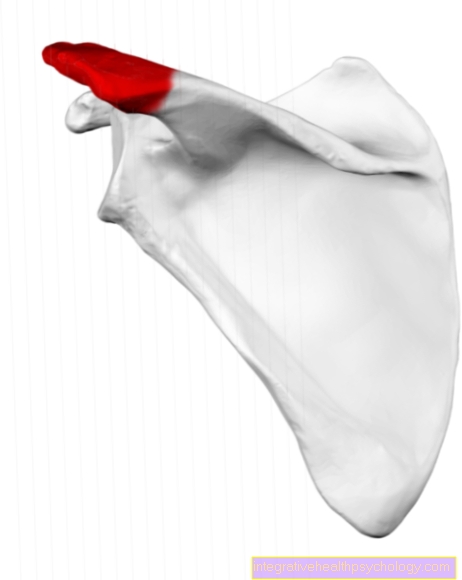
In the last section, the supply of the menisci via the joint capsule was briefly discussed. At this point, this should be presented in more detail. A distinction is made morphologically (= regarding the cellular structure) the meniscus base, which is more directly connected to the joint capsule (red zone), from the middle meniscus area (light red zone) and the white edge zone. Vessels penetrate through the red zone into the middle third of the meniscus (marked in light red). The white border, however, has no vessels. It is supplied by the synovial fluid (= synovial fluid). These findings have a major impact on the chances of recovery for various meniscal injuries. While the chances of recovery are good for the red and light red areas due to the supply through the vessels, a meniscus tear in the area of the white border is much more difficult to treat. A healing in the strict sense (restoration of an uninjured meniscus) is not possible in this zone.
Since the cartilage is an important part of the knee joint, which can be damaged in particular by torn / torn menisci, the function of the cartilage should be discussed at this point:
The cartilage represents a supporting tissue, which consists of water-rich cartilage cells (= chondrocytes) and so-called intercellular substances (basic substance, fibers). Depending on the nature of the intercellular substance, a distinction is made between:
- hyaline cartilage
- elastic cartilage
- Fibrous or connective tissue cartilage
While cartilage can be found in many areas of the body, the hyaline, but also the fibrous or connective tissue cartilage (= mixture of collagen and hyaline cartilage) is of particular importance for the knee. When the cartilage has been used up through excessive wear and tear or injury, the body can neither repair nor synthesize this cartilage tissue. The doctor then speaks of the clinical picture of arthrosis (You can find more on this in the definition of terms arthrosis).

In the knee joint area, the meniscus makes a special contribution to protecting the cartilage. The meniscus dampens impacts, but also stabilizes the knee in a special way in cooperation with the cruciate ligaments. In MRI video sequences it could be proven that the band connections of the menisci in particular are required for the shock absorber function. Loosened / torn ligament connections can also be made responsible for meniscus tears, which may develop from superficial meniscus tears. The yellow arrow indicates a healthy meniscus.
Torn or torn menisci destroy the cartilage tissue in that they can no longer or fully exercise the shock absorber function. A Osteoarthritis of the knee joint as a serious consequence can and will occur sooner or later.
Studies have shown that meniscus injuries occur more frequently in the area of the inner meniscus, regardless of their cause. The area of the posterior horn is particularly susceptible to injuries (approx. 75% of all injuries to the inner mensis affect the area of the posterior horn).
You can also find more information about the anatomy of the meniscus under our topic Meniscus.


.jpg)