Adrenal gland
Synonyms
Glandula suprarenalis, glandula adrenalis,
engl.: adrenal gland
definition
The adrenal glands are important hormonal glands in the human body. Everyone has 2 adrenal glands. The adrenal gland rests on the kidneys from above like a kind of cap and is around 4 cm long and 3 cm wide with an average weight of 10 grams.
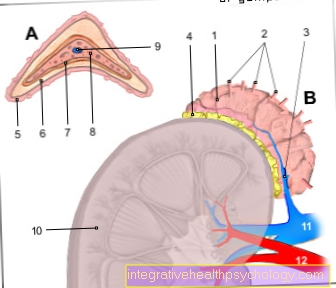
Structure of the adrenal gland
The organ can be roughly divided into two sections:
The inner adrenal medulla (Medulla glandulae suprarenalis) is functionally part of the likeable Nervous system, because here the hormone or the carrier substance adrenaline and Norepinephrine, also Catecholamines called, are formed. The adrenal medulla is drawn from the outside by the adrenal cortex (Cortex glandulae suprarenalis), which has important functions in the body's hormonal balance. It also represents the main part of the organ and is exposed to the outside by a connective tissue capsule (Capsula fibrosa) limited. The adrenal cortex can in turn be divided into three sections according to the function and arrangement of the cells: from the outside to the inside there is the zona glomerulosa (Ball-like or ball-like arrangement of the cells), Zona fasciculata (columnar arrangement) and Zona reticularis (net-like arrangement).The adrenal cortex is able to intervene in the body's water, sugar and mineral balance through the hormones it produces. The hormones synthesized by the adrenal cortex all belong to the group of Steroid hormonesbecause they have the same precursor molecule cholesterol (basic chemical structure of sterane) own.
Illustration adrenal gland and kidney
- Adrenal gland -
Glandula suprarenalis - Adrenal arteries -
Suprarenal artery - Adrenal vein -
Suprarenal vein - Fat capsule -
Capsula adiposa
(5th-7th adrenal cortex
C.ortex) - Ball zone -
Zona glomerulosa - Bundle zone - Zona fasciculata
- Grid zone - Zona reticularis
- Adrenal medulla - Medulla
- Central vein - Central vein
- Right kidney - Ren dexter
- Renal vein - Renal vein
- Renal artery - Renal artery
You can find an overview of all Dr-Gumpert images at: medical illustrations
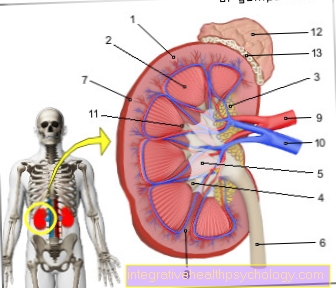
- Renal cortex - Renal cortex
- Renal medulla (formed by the
Kidney pyramids) -
Medulla renalis - Kidney bay (with filling fat) -
Renal sinus - Calyx - Calix renalis
- Renal pelvis - Pelvis renalis
- Ureter - Ureter
- Fiber capsule - Capsula fibrosa
- Kidney column - Columna renalis
- Renal artery - A. renalis
- Renal vein - V. renalis
- Renal papilla
(Tip of the kidney pyramid) -
Renal papilla - Adrenal gland -
Glandula suprarenalis - Fat capsule - Capsula adiposa
You can find an overview of all Dr-Gumpert images at: medical illustrations
Diseases of the adrenal cortex
A general distinction is made between over and under-functioning of the adrenal gland, depending on whether too much or too little hormone is produced. The causes are varied.
For detailed information on overactive adrenal gland, see: Overactive Adrenal Glands - Symptoms, Duration & Treatment
Overproduction of aldosterone = Conn's syndrome
Conn's syndrome (also primary hyperaldosteronism) there is an increased production of aldosterone in the Zona glomerulosa based on the adrenal cortex. This is mainly caused by benign tumors, also called adenomas, or a simple enlargement (Hyperplasia) the zona glomerulosa, the cause of which has not yet been clarified. The increased supply of aldosterone leads to an increase in blood pressure and a decrease in the potassium level in the blood. This usually leads to headaches, muscle weakness, constipation and increased and frequent urination, often at night (Polyuria, nocturia), as the flushed-out potassium draws water with it. In addition, patients often complain of an increased feeling of thirst (Polydipsia). The shift in the potassium balance can also lead to cardiac arrhythmias. However, there is also a form of the disease in which the potassium level is not changed, i.e. in the normal range.
If the disease is based on a tumor, the symptoms can be dealt with by surgical removal. Is it a Hyperplasia, one gives aldosterone antagonists that counteract the effect of the body's own aldosterone, such as Spironolactone. In addition, the blood pressure usually has to be brought into the normal range using suitable medication.
Overproduction of cortisol = Cushing's disease
Cushing's disease is caused by an increased production of cortisol from the Zona fasciculata the adrenal cortex. This occurs, for example, with tumors Pituitary gland in front. The tumor produces an increased amount of the hormone ACTH, which stimulates the adrenal cortex to produce cortisol. Other causes are an enlargement of the adrenal gland, either from a tumor or from increased bilateral growth (Hyperplasia). The symptoms that the patients then show are also summarized under the name Cushing's syndrome and are relatively characteristic of the disease: the patients suffer from trunk obesity with fat accumulation on the trunk, especially in the abdominal area, while the arms and legs are very thin. In addition, there is often a thickened neck ("bull neck") and a round face ("moon face"). Patients' skin is similar to parchment paper in that it often becomes very thin and the bones become brittle (osteoporosis). Above all, the carbohydrate metabolism is disturbed, which can lead to diabetes with increased thirst and increased urination.
Long-term administration of cortisone as a drug can also lead to Cushing's disease. It is therefore important to ensure that the patient only takes this medication for as long as necessary. A tumor should be removed for treatment if possible. If this is not the case, drugs are given that inhibit the overproduction of cortisol.
Read more on the topic: Cushing's disease
Underactive adrenal cortex = adrenal insufficiency
If the adrenal cortex does not produce sufficient cortisol, it is called adrenal insufficiency. Depending on where their cause lies, a distinction is made between a primary, a secondary and a tertiary form.
If the cause lies in the adrenal cortex itself, one speaks of primary adrenal insufficiency or Addison's disease. In most cases, this is caused by autoimmune reactions against cells of the adrenal cortex, but it can also be caused by certain infectious diseases such as Tuberculosis or AIDS. Tumors can also be responsible for this. The pituitary gland reacts to the decreased supply of cortisol via a feedback mechanism with an increased release of ACTH. However, the ACTH-producing cells in the pituitary gland also produce another hormone: MSH (melanocyte-stimulating hormone). This hormone stimulates the skin's melanin-producing cells to produce pigment. So it happens that patients with Addison's disease usually have a heavily tinted skin.
If the cause is outside the adrenal gland, it is called secondary or tertiary adrenal insufficiency. This is the case with diseases of the hypothalamus (tertiary) or the pituitary gland (secondary), which are then no longer able to produce sufficient CRH or ACTH, which means that the adrenal cortex receives too few stimuli for cortisol production. This can be the case with tumor diseases, inflammation and other diseases in these areas of the brain. But symptoms are also possible after cortisone therapy has been discontinued too quickly: the long-term administration of Corstison has made the body used to high blood Corstison levels. The pituitary gland hardly releases any ACTH. If the treatment is stopped very quickly, the hypothalamus and pituitary gland cannot get used to it so quickly. The body then quickly lacks cortisol. It can lead to a "Addison crisis“Come with a rapid drop in blood pressure, vomiting and shock. Therefore, care should always be taken to slowly taper off cortisone therapy in order to give the body the opportunity to supply itself with the necessary hormone dose again.
Possible symptoms that adrenal insufficiency can cause are: lack of drive, low blood pressure, nausea with vomiting, fatigue, weight loss, loss of pubic hair and dizziness. However, many symptoms appear very late in the course of the disease, so that large parts of the adrenal gland are often destroyed. The therapy of choice is a substitution of the missing hormones.
You can also find out more about Addison's disease under our topic: Addison's disease and Addison's crisis.
What might also interest you: Symptoms of low blood pressure
Adrenal medulla disorders
Pheochromocytoma
The pheochromocytoma is a mostly benign tumor (about 90%), the catecholamines (Norepinephrine and adrenaline) produced. In the majority of cases it is located in the adrenal medulla, but it can also be located in other parts of the body, e.g. in the trunk, a plexus of nerves that runs parallel to the spine. Due to the increased and uncontrolled release of adrenaline and above all noradrenaline, patients with pheochromocytoma suffer from permanent increases in blood pressure, or from seizure-like high blood pressure crises, in which life-threatening values can be reached, as cerebral hemorrhage or heart attacks can no longer be ruled out. Concomitant symptoms are excessive sweating, dizziness, headache and palpitations.
The pheochromocytoma is usually discovered quite late. The method of choice if this disease is suspected is the determination of the catecholamines in the urine and in the blood. The therapy of choice is surgical removal of the tumor, which may be accompanied by removal of the adrenal gland.
Read more on this topic at: Pheochromocytoma
Underactive adrenal medulla
An underfunction of the adrenal medulla is also possible, but rarely, e.g. after surgical damage to the adrenal gland. If enough catecholamines are no longer produced, the body has difficulty maintaining blood pressure. This can lead to dizziness and fainting spells. Means to increase blood pressure are used therapeutically.
Waterhouse-Friedrichsen Syndrome
At the Waterhouse-Friedrichsen Syndrome it is an acute failure of the adrenal glands after a massive infection with meningococci, Haemophilus influenzae or pneumococci.
Consumption coagulopathy occurs: due to excessive blood clotting with blood clot formation, the factors necessary for blood clotting are used up, which leads to heavy bleeding, especially in the adrenal gland. Since the adrenal glands are no longer functional, immediate administration of hydrocortisone and catecholamines is essential.
You can find further information under our topic: Waterhouse-Friedrichsen Syndrome