Neocortex
Synonyms
Neocortex, isocortex
definition
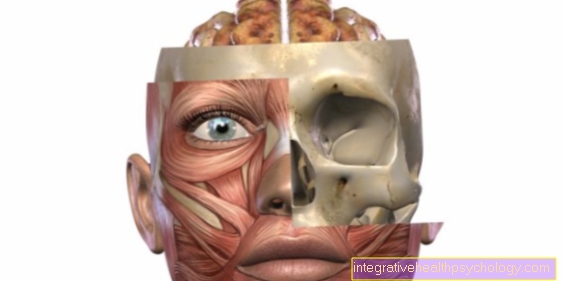
In terms of developmental history, the neocortex represents the youngest part of the brain. It can be divided into four brain lobes that take on different brain functions.
Frontal lobes
Anatomy & function:
The frontal lobe plays the central role in the initiation of motor skills.
In the motocortex (Precentral gyrus) the movements are "designed". It is structured somatotopically. This means that a specific part of the body is assigned to each area of the motocortex. The hand, face and tongue are represented clearly disproportionately.
The motocortex transmits its information via the Pyramidal track towards peripheral. Before that, however, the information is still in for fine-tuning and coordination Cerebellum and Basal ganglia.
That too motor language center (Broca area) lies in the frontal lobe. However, only in the dominant, usually the left, hemisphere.
It is indispensable for language production and understanding and is closely related to the Wernicke area (see below) linked in the temporal lobe.
clinical evidence:
A lesion in the area of the motocortex causes one paralysis (Paresis) on the opposite side of the body, as a large part of the pyramidal path crosses on its way from central to peripheral to the opposite side.
A lesion in the area of the Broca area leads to Broca's aphasia. Those affected can understand what is said and written, but speaking and writing is much more difficult.
Often only single chopped off words can be formulated.
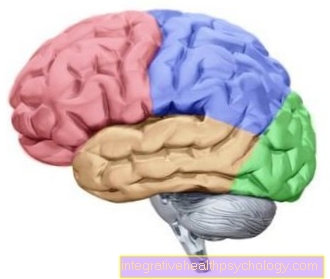
Brain lobe
Frontal lobe = red (frontal lobe, frontal lobe)
Parietal lobe = blue (parietal lobe, parietal lobe)
Occipital lobe = green (occiptital lobe, occipital lobe)
Temporal lobe = yellow (temporal lobe, temple lobe).
Parietal lobes
Anatomy & function:
Above all, sensitive stimuli are integrated and processed in the parietal flap.
This is how the information reaches Protopathy (Pain, temperature, gross tactile sensation) and Epicritic (fine touch and proprioception) after passing through the thalamus into the postcentral gyrus, where the primary somatosensitive cortex lies.
This lies against the gyrus precentrealis of the frontal lobe, in which the motor function is generated.
Information about touch or other sensitive stimuli that have arrived in the primary somatosensitive cortex is perceived as such, but not yet interpreted.
This only happens in secondary somatosensitive cortex.
The parietal lobe also includes - among other regions - the Angular gyrus. He is the switching point between secondary visual cortex and sensory language center, i.e. the Wernicke area. It is essential for reading and writing.
clinical evidence:
The sensitive pathways also cross - like the motor ones - on their way from peripheral to central at some point on the opposite side.
Accordingly, a lesion results in the area of the primary somatosensitive cortex to a failure of the function in the opposite (contralateral) Half of the body.
The affected person no longer feels anything in the corresponding part of the body.
If there is a lesion in the secondary somatosensitive cortex however it comes to tactile agnosia. Objects that have been touched are no longer recognized.
This is because the secondary sensitive cortex is not responsible for the perception of what is felt but for its interpretation.
A lesion of the Cingulate gyrus leads to reading disorders (Alexia) and / or writing (Agraphy).
Occipital lobe
Anatomy & function:
The visual center, i.e. part of the visual system, is located in the occipital lobe, which is located in the posterior fossa above the cerebellum.
The information comes from the retina (retina) via the optic nerve (Optic nerve, 2nd cranial nerve) into the optic chiasm (Optic nerve junction), where the information of the outer (lateral) Cross the visual field on the opposite side.
The fibers continue to run in the optic tract, whereby through the junction in the chiasm the right optic tract provides information about the inner (medial) Contains the visual field of the right and the lateral visual field of the left eye.
The fibers run through the corpus geniculatum mediale in the thalamus and as visual radiation to the primary visual cortex in the occipital lobe. It lies in the area of the calcarin sulcus.
If the information from the eye reaches the primary visual cortex, the person becomes aware that he is seeing something, but the visual impression is not yet interpreted. This only happens in the secondary visual cortex, which is adjacent to the primary one.
clinical evidence:
Lesions in the area of the visual system can be caused by a wide variety of causes, for example inflammation, trauma or tumors.
The symptoms of such a lesion can also vary greatly depending on the location. For example, a lesion of the primary visual cortex on only one side leads to loss of vision on the medial side of one eye and the lateral side of the other eye (homonymous hemianopia).
Lesions in the peripheral area of the visual pathway also lead to, mostly relatively characteristic, visual field defects.
If, on the other hand, the secondary visual cortex is affected, this does not lead to visual field defects or blindness.
The patients can still see, but they can no longer interpret what they see (visual agnosia).
An example is the failure to recognize faces when the eyesight is intact (Prosopagnosia).
Temporal lobe
Anatomy & function:
The central part of the auditory system, i.e. hearing, is located in the temporal lobe.
The information is transmitted via the auditory nerve cells in the Inner ear to nerve cell nuclei in the Medulla oblongata (Nuclei cochleares) forwarded.
There is a tonotopic structure, i.e. a structure of the information according to height and frequency. This is also found in the cerebral cortex.
Most of the nerve fibers cross after passing through the Medulla oblongata on its way into the cerebral cortex on the opposite side, the small part continues on the same side.
The path continues to the upper olive stones and then as Lemniscus lateralis continue to the Inferior colliculi the quadrilateral plate of the midbrain.
From here the nerve fibers run on to the Corpus geniculatum mediale of the thalamus and from there as hearing radiation to primary auditory cortex in the area of the Heschl transverse turns of the temporal lobe.
In this way, smaller fiber groups cross from one side to the other, so that the primary auditory cortex on one side provides information about what has been heard Cochlea (Cochlea) on both sides, this is essential for directional hearing.
in the primary auditory cortex the listener becomes aware of what has been heard, but without it being interpreted.
This only happens in the secondary auditory cortex. Once the information has arrived and processed, the sounds heard are recognized as words, melodies or noises, for example.
It is interesting that the secondary auditory cortex of the dominant hemisphere, in which the Broca language center is also located, is primarily responsible for the processing, recognition and understanding of language. It is therefore also called sensory language center or Wernicke area.
The secondary auditory cortex of the non-dominant hemisphere, on the other hand, processes things like melodies. So it is crucial for understanding and recognizing music.
clinical evidence:
A lesion of the primary auditory cortex one side does not lead to deafness but to a decrease in hearing in both ears.
This is because the nerve fibers are on the way from Inner ear Cross into the cerebral cortex several times on the opposite side and one side of the brain receives information about what is heard from both ears.
However, this also means that if the primary auditory cortex is disturbed on one side, directional hearing is significantly more difficult.
With a lesion of the secondary auditory cortex The symptoms depend very much on whether the dominant or the non-dominant hemisphere is affected.
In the event of damage to the Wernicke area, that is the secondary auditory cortex of the dominant hemisphere, the speech understanding of those affected is severely impaired. They often talk a lot (Logorrhea) but without any sense to the outsider. In doing so, they are not aware that what they are saying does not make sense.
A lesion the secondary auditory cortex in the non-dominant hemisphere however, results in a loss of music understanding, but does not affect speaking.



.jpg)