Neuroma
Synonym
Schwannoma, Neurilemmoma, Benign Peripheral Nerve Sheath Tumor (BPNST)
Engl .: neurinoma
introduction
The Neuroma is a slowly growing, benign tumorwhich is usually surrounded by a connective tissue capsule and grows displacingly, i.e. does not infiltrate the surrounding tissue. It is derived from so-called Schwann cells of the peripheral Nervous system and arises on the cranial and peripheral nerves annoy.

Epidemiology
6-7% of all Brain tumors are neuromas, spinal neuromas are the most common spinal ones Tumors with 25%. The acoustic neuroma is the most common neuroma, around 80% of all tumors in the cerebellopontine angle are acoustic neuromas.
About 10% of patients with type 2 neurofibromatosis develop a neurinoma; the incidence of type 2 neurofibromatosis is 1 in 50,000.
The age of onset is between the ages of 30 and 50, women are affected slightly more often than men.
causes
The cause of a Neuroma is generally unknown. The most common known cause is neurofibromatosis type 2, very rarely also neurofibromatosis type 1.
In the Neurofibromatosis type 2 there is a mutation of a gene on chromosome 22, a so-called NF-2 mutation, which is inherited dominantly. Their frequency is 1:50 000. In neurofibromatosis type 1 (NF-1) there is a defect on chromosome 17. It makes up 90% of neurofibromatoses and is also a dominant hereditary disease with a frequency of 1: 2000-3000. It is derived from the Schwann cells of the peripheral nervous system.
Appearance
A Neuroma is a connective tissue encapsulated tumor with a light, yellowish cut surface. The tumor cells are elongated and thin, their cell nuclei are pushed together in a row formation (Palisade position).
Two types of tissue patterns can be distinguished microscopically:
- Antoni-A-Formation: fiber-rich and elongated cells with narrow, cigar-shaped nuclei that form trains, vertebrae and parallel rows of nuclei.
- Antoni-B formation: low in fibers, net-like with often altered tissue changes such as fat deposits. The cell division activity is very low.
Occurrence
A Neuroma can occur in all sections of the peripheral nervous system, preferred locations are the Cerebellar bridge angle (Acoustic neuroma) or the sensitive nerve roots in the Spinal cord (spinal neuromas).
Acoustic neuromas originate from a part of the auditory and equilibrium nerves (Vestibulocochlear nerve, VIII. Cranial Nerves) and arise at the exit point of the nerve from the Brain stem. This section of nerve is located in a canal in the base of the skull, called the Canalis acusticus internuswhere the wrapping of the peripheral nerve with the Schwann cells begins. Schwann cells are cells in nerve tissue that form envelope and supporting cells that encase and electrically isolate the extension of a nerve cell.
Spinal neuromas can develop at any level of the spinal cord, but are most commonly located in the upper and middle cervical and upper thoracic cords, and can extend longitudinally over several segments. During the expansion, there is often an intraspinal, i.e. in the spinal canal, and extraspinal, i.e. lying outside the spinal canal, which are connected by a narrow bridge (Hourglass swelling). Spinals Neuromas also often come often (multiple), especially with neurofibromatosis type 2 (see causes).
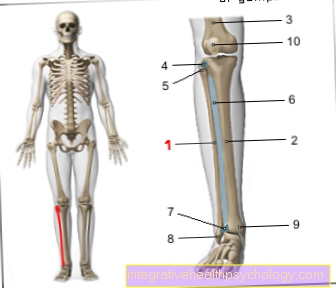
Lumbar spine neuroma
Since the neuroma originates in the envelope cells of a nerve, it can also be located in the lumbar spine (lumbar spine) area. The problem is then that even if the tumor grows slowly, the one next to it Nerve compressed becomes. The pressure then damages the nerve cells. The result is back pain that radiates into the leg, so-called Lumboischialgia. This can easily be done with typical sciatic complaints be confused.
Read about this: Pinched sciatic nerve
Often the patients also notice sensory disorders in the leg area. If the tumor continues to grow, the muscles supplied by the nerve may become weak.
The diagnosis can be made using MRI of the lumbar spine be asked. Already in the x-ray of the spine you can often see that the lateral opening, i.e. the bony window to the spinal canal, is widened by the tumor growth. Here, too, the following applies: if symptoms exist, microsurgical removal of the tumor makes sense.
Neuroma of the cervical spine
The neuroma can also occur in the cervical spine (Cervical spine). Here, too, the problem is that the tumor grows only slowly, but can compress adjacent nerves. The pressure then damages the nerve cells. The consequences are then Pain in the cervical spine with radiation in the arm or sensory disturbances.
If the tumor continues to grow, the muscle supplied by the nerve can also become weak. The diagnosis can be made using MRI of the cervical spine be asked. Here, too, the following applies: if symptoms exist, microsurgical removal of the tumor makes sense.
Neuroma in the spinal canal
The problem with a neuroma in the spinal canal is that space in the spinal canal is limited. As the neuroma grows, it comes to Displacement of the spinal cord. This can damage the nerve fibers running there. The result is usually referred pain in the arms or legs as well as sensitivity disorders.
The diagnosis is made by means of cross-sectional imaging (MRI of the spine or CT). In the event of complaints, the neuroma should always be surgically removed.
Neuroma on the foot
Neuromas can develop anywhere in the peripheral nervous system. In addition to the frequent growth in the head and neck region, the extensor sides of the extremities or the spinal / cranial nerves, a neurinoma can develop on the foot in rare cases.
Clinically, this usually shows a rough, nodular nerve change on the foot. This is typically pressure and touch sensitive and can sometimes cause massive pain. In addition, patients often report a permanent tingling sensation and numbness in the area covered by the damaged nerve. This is because the growth of a neuroma in the area of the nerve sheath can irritate or compress the nerve that runs next to it. This irritation of the nerve can be aggravated by touch or movement.
The neuroma on the foot should be differentiated from Morton's neuralgia. Continuous pressure or a misalignment of the foot lead to a reactive increase in the tissue in the area of the nerve. As a result, the neighboring nerve can also be compressed and damaged.
Neuroma on the finger / hand
Since the neuroma can in principle occur on all nerve fibers in the body, a neuroma can also be localized on the finger or in the hand. The problem here too is that even if the tumor grows slowly, the adjacent nerve is compressed.
Symptoms in neuromas on the finger or hand are usually one painful tingling sensation or a Numbness in the supply area of the damaged nerve. This can be determined with a simple clinical test. Tapping the nerve leads to the above-described abnormal sensations. One then speaks of a positive Hoffmann-Tinel sign, which is also the case with one Carpal tunnel syndrome occurs.
Here, too, a must to confirm the diagnosis MRI of the hand be performed. The tumor should then be removed by a hand or neurosurgery. As part of a microsurgical procedure, the tumor is carefully peeled off from the affected nerve. The postoperative results are often very good.
Acoustic neuroma
The acoustic neuroma is a benign brain tumor. It arises from the envelope cells of the 8th cranial nerve. This is the auditory and balance nerve. Acoustic neuromas are among the most common tumors in the skull. Usually they just kick one-sided on. If the tumor exists on both sides, one should think of neurofibromatosis type 2.
Patients with acoustic neuroma typically have the following symptoms: Hearing loss, Balance disorders with dizziness, such as Tinnitus.
The diagnosis can be made using MRI or CT. Also a special hearing test (BERA) to measure the hearing ability on the brain stem makes sense.
The therapy the choice should always be surgical removal. If you operate at an early stage, the function of the nerve can largely be preserved. Another therapy option is radiation therapy. This is decided if the tumor is inoperable or the age or general condition of the patient does not allow an operation. If the tumor has been completely removed, the prognosis is very good. Life expectancy is not restricted.
Symptoms
The Neuroma itself is movable and not painful.
A hearing loss (Hypacusis) is the most common symptom and is decreasing due to the slow growth of the Neurinoma a creeping course. Occasionally the patients complain of hearing impairments when using the telephone and describe a change in their telephone habit with switching to the other ear. Other early signs are ringing in the ears (Tinnitus), dizziness in the event of a quick change of position and uncertainty in the event of a quick turn around.
In the further course it comes to permanent dizziness, disturbances of the Movement coordination (Ataxia), especially unsteady gait and a spontaneous, rapid return movement of the Eyeball (Spontaneous nystagmus). As the tumor continues to grow, the cranial nerves, the brain stem, and the cerebellum are pinched. When the facial nerve (Facial nerve) is affected, it can lead to paralysis of the mimic Musculature (Facial palsy) come. When the triple nerve (Trigeminal nerve) is affected, facial numbness, spontaneous attacks of pain in the head area (Trigeminal neuralgia) and taste disorders come. When the cerebellum is narrowed, ataxia occurs; when the brain stem is narrowed, it increases Intracranial pressure and characteristic intracranial pressure symptoms occur (nausea, Vomit, etc.). Also the 4th ventricle, a cavity of the brain-Spinal fluid (Cerebrospinal fluid), can be narrowed. This leads to a congestion and thus to a disruption of the CSF circulation, which, however, occurs rarely and only in very large tumors.
Neuromas The nerve roots of the sensory nerves usually pinch in the spinal canal. The patient has unilateral, radiating (radicular) Pain in the skin area belonging to the respective sensitive nerve (Dermatome). The pain intensifies as the pressure in the spinal canal increases until it decreases again and ultimately even stops when the root of the sensory nerve is completely destroyed. In the further course it can slowly become asymmetrical Paraplegia develop, albeit the nerve roots of the annoy pinched, which control muscle movement (motor nerves).
Pain as a symptom
The neuroma is not painful in itself. However, due to its suppressive growth in the area of the nerve sheath, there is always the risk that the adjacent nerve will be compressed or irritated. As a result, the patient may experience very severe pain.
These typically also occur at rest, as the tumor presses permanently on the nerves. Touching the nodular mass of the tumor or putting it under strain can intensify the pain stimulus.
Treatment with painkillers can temporarily relieve the pain, but surgical removal of the tumor is usually necessary in the case of severe symptoms.
diagnosis

For an accurate diagnosis and to plan the subsequent treatment, imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI of the head) used. This involves taking layer images of the entire body from the top of the head to the feet, which are then put together to form an entire three-dimensional image.
An indirect indication of a neuroma is the expansion of the Internal acoustic canal, what in CT can be seen. In general, however, it is very difficult to differentiate between nerve and tumor tissue in CT. That's why this is MRI of the brain the method of choice for the detection of neuromas and for the representation of the spatial extent of cerebellar bridge angle tumors.
Another important point for the diagnosis is a significant increase in the protein content in the Liquor.
When diagnosing hearing disorders, it should be borne in mind that only 5% of these patients have an acoustic neuroma. The diagnosis of hearing impairment is made using audiometry, and calorimetry aacoustic evoked Ppotential (AEP) determined. For example, the reaction of the auditory cells and the various stations of the auditory pathway in the brain to acoustic stimuli is measured.
MRI for a neuroma
Magnetic resonance imaging (MRI) is the method of choice for diagnosing neuroma.
In a computed tomography (CT) it is difficult to differentiate between the neuroma and the surrounding tissue. This contrast is better in the MRI examination. The administration of contrast medium enables the size of the tumor to be assessed even better, since the contrast medium accumulates in the neuroma.
Compared to other tumors in the area of the peripheral nervous system, neuromas often show a cystic appearance (several cavities) and a fatty remodeling of the tissue. Bleeding may also occur, which can be easily assessed with the aid of the administration of contrast medium.
therapy
If there are no complaints and that Neuroma is still very small, the tumor does not have to be treated. However, it should be closely monitored through regular check-ups using MRI.
Radiation therapy can be used for smaller neuromas, but usually the tumor is completely surgically removed, which leads to healing. The neuroma does not develop again after the operation. The death rate from this type of surgery is less than 5%, mostly affecting elderly patients with risk factors. The facial nerve can be preserved in 90% of patients and hearing, depending on the tumor size, in around 60% of patients. Paralysis and bladder disorders recede well, sensitivity disorders only partially.
Malignant degenerate neuromas must be irradiated after the operation and can form daughter tumors (metastases) in other parts of the body.
Rehabilitation / prognosis

Most patients are cured after successful therapy and can go back to work.
The Neuroma grows very slowly over several years and initially goes unnoticed. Depending on the size of the tumor, hearing cannot be preserved in around 40% of patients (Anacusis), in around 10% of patients the Facial nerve are not preserved and the facial nerve palsy persists. The prognosis is worse if the tumor was detected too late and the spinal cord has been pinched (spinal cord compression) in spinal neuromas for a long time.
Malignant degeneration of the tumor rarely occurs, and that too Metastases can form outside the peripheral nervous system. These malignant neuromas correspond to tumors III. or IV. degree and are also known as neurofibrosarcomas and neurogenic sarcomas. The prognosis for these types of tumors is much worse.
Neuroma and Schwannoma - What's the Difference?
A neuroma is a slowly growing, benign tumor of the peripheral nervous system. It develops from the so-called Schwann cells, which are responsible for the formation of the nerve sheaths.
There is no difference between a neuroma and a schwannoma. The term "neuroma" is used more frequently in everyday clinical practice, although "schwannoma" is actually more appropriate due to the tissue of origin (Schwann cells).
Summary
A neuroma is a benign new growth in Schwann cells. The most common type of neuroma is the acoustic neuroma. In this type there is progressive hearing loss (Hypacusis), Ringing in the ears and balance disorders. As the tumor grows, other cranial nerves fail, leading to facial paralysis and numbness of the face.
With further increase in size, the cerebellum and brain stem can also be affected, which in particular leads to ataxia. The increase in protein in the liquor is diagnostically important. The treatment of choice is the complete surgical removal of the tumor.