Pheochromocytoma
Synonyms in a broader sense
Adrenal tumor
English: pheochromocytoma, pheochromoblastoma
definition
A pheochromocytoma is a tumor that produces hormones (usually adrenaline and noradrenaline). In 85% of cases, the tumor is in the adrenal gland.
In most cases (85%) the tumor is benign, 15% are malignant. Usually (90%) the pheochromocytoma is unilateral, but 10% are bilateral.
Furthermore, the pheochromocytomas are differentiated based on the hormones that they produce. Around 2/3 produce adrenaline and noradrenaline. Malignant tumors are characterized by their additional dopamine production.
Pheochromocytoma is an example of a congenital disorder associated with overactive adrenal glands. The overactive adrenal glands can have serious consequences for the body. Find out more about this topic at: What are the consequences of an overactive adrenal gland?
Summary
A pheochromocytoma is a tumor, usually located in the adrenal gland, which produces the hormones adrenaline and noradrenaline.
Most often it is a benign tumor.
If the tumor also produces dopamine, it is malignant. This hormone production causes the patient's blood pressure to rise. Other symptoms include palpitations, paleness and sweating. In addition to the symptoms, various tests and imaging procedures are used for diagnosis. Surgical removal of the tumor is the focus of therapy. The symptoms alone can also be treated with medication.
There is no prophylaxis. The prognosis depends on the dignity (benign or malignant) of the tumor.
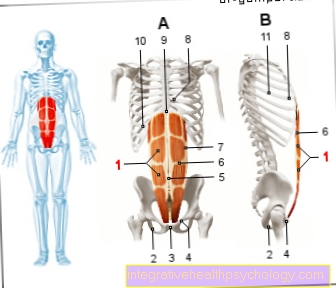
Figure adrenal glands
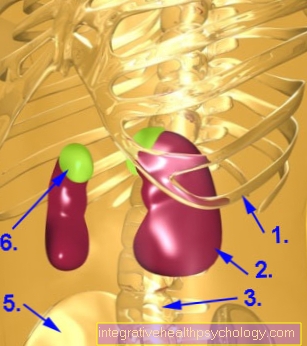
- Ribs
- kidney
- Spine
- the author can't count :-)
- pool
- Adrenal gland
The adrenal gland is located at the so-called upper pole of the kidney and, as you can see, it is significantly smaller than the kidney.
causes
The cause of the high blood pressure can be explained as follows:
Since the tumor is mostly in the Adrenal gland is found, the result is high blood pressure. The adrenal medulla produces adrenaline and Norepinephrine.
The cells of the adrenal medulla grow uncontrollably in a pheochromocytoma. The tumor produces the same hormones (adrenaline and noradrenaline) that are produced when the sympathetic nervous system (The sympathetic nervous system is part of the so-called autonomic nervous system, which, without deliberately influencing it, controls many parameters such as blood pressure, sweat i.a. regulated) increase blood pressure.
Norepinephrine increases blood pressure by reducing it smooth musculature the arterial vessels to contraction. Adrenaline, on the other hand, changes the blood pressure by increasing the minute volume (volume, which from Heart in one minute) of the heart. It also speeds up the heartbeat.
We are currently trying to explain why the pheochromocytoma itself develops as follows:
The assumption that about 10% of these tumors occur in families is confirmed. A certain hereditary component that is in our genes is therefore of certain importance in the development of the tumor and the onset of the disease.
Symptoms / complaints
The blood pressure increases, which either remains at a relatively constant level or is accompanied by highs (blood pressure peaks) and lows.
Especially when the blood pressure soars, the patient complains of:
- a headache
- sweat
- Palpitations
- Tremor (tremor)
Other important symptoms are pale skin and weight loss !! An increased number of white blood cells can be detected in the blood count.
If the face is reddened and weight has been gained, this speaks against the diagnosis of pheochromocytoma.
diagnosis
The diagnosis is based on the one hand on the clinic (symptoms / complaints), on the other hand using laboratory tests and imaging diagnostics (MRI / CT).
In addition to the above symptoms (a headachePalpitations, palpitations), the doctor may make the following findings:
In the 24h blood pressure measurement, the physiologically actually present lowering of blood pressure overnight is missing.
It takes a measurement of the Hormonesthat are typically formed by pheochromocytomas take place. It can be measured either in the urine or in the blood.
Either the hormones themselves or their breakdown products (e.g. vanellin almond acid) are measured in the 24-hour urine. Values over 200 ng / l to have disease valueas long as the hormones are below a value of 50 ng / l lie, they are called normal classified.
Values above apply in the blood 2000 ng / l as pathological (morbid), Values below 500 ng / l are normal.
Then, if pheochromocytoma is suspected, the hormone can also be used Dopamine to be determined. (Dopamine is usually only obtained from malignant tumors of this type - apart from the body's regular dopamine production, of course).
To get a backup of the diagnosis, a confirmation test is carried out. This is done by the patient Clonidine, a centrally acting agent against high blood pressure, applied (administered). Normally the concentration of now drops Catecholamines (Adrenaline and noradrenaline) in the blood. However, this does not happen with autonomous catecholamine erosion due to a pheochromocytoma.
A comparative measurement between the amount of hormones in the daytime urine and the amount in the nighttime urine (after administration of clonidine) also helps to establish the diagnosis. At night - urine usually shows up in healthy patients, but also in patients with primary hypertension (not caused by another disease high blood pressure), a sharp drop in catecholamines. If this is not the case, then there is a pheochromocytoma.
A localization of the pheochromocytoma is through imaging diagnostics, such as Ultrasonic, Computed tomography (CT) or Magnetic resonance imaging (MRI) possible.
therapy
As is so often the case, there are two different therapy methods that can be used. The decision which is more suitable must be made individually. As a rule, depending on the extent of the tumor and the disease, conservative treatment is attempted. However, the size and ingrowth into the surrounding tissue can also stand in the way of an operation. Even so, it comes first.
surgery
If the pheochromocytoma is only on one side, the entire adrenal gland is removed. If the disease is bilateral, an attempt is made to partially preserve the adrenal gland in order to spare the patient hormone replacement therapy.
Conservative treatment
First, the disease is treated by trying to relieve the symptoms, i.e. lowering blood pressure. This is done with various antihypertensive drugs (drugs against high blood pressure).
If there is an inoperable tumor, will Medication administered, which the synthesis (structure) of catecholamines (adrenaline and Norepinephrine) inhibit.
Does the tumor already have metastases (Daughter tumors), then usually only the chemotherapy.
prophylaxis
Since no specific factors are known for the development of the pheochromocytoma that favor the growth or onset of the disease. Accordingly, prevention can hardly be done.
Only members of predisposed families should consider genetic counseling to see if preventive tests can be performed. The probability of falling ill can also be roughly calculated in a genetic counseling center.
forecast
The prognosis is different. After the tumor is surgically removed, it occurs at 80% of patients who had benign pheochromocytoma to one normal blood pressure.
In all other patients with a removed benign tumor there is a so-called essential hypertension in front. So the blood pressure is still high because of other causes.
In benign tumors, the 5th - annual survival rate at about 95%. If there is a malignant tumor that has already spread metastases (daughter metastases), the 5-year survival rate is only 44%.














.jpg)