Shoulder joint instability
introduction
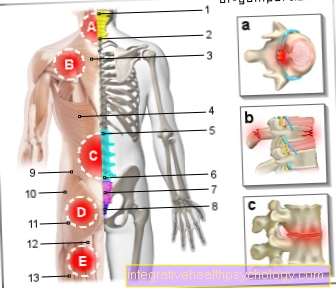
Instabilities tend to occur in the shoulder joint, which can be explained by the anatomy of the shoulder joint. The relatively large head of the humerus stands on a much smaller shoulder joint socket (Glenoid), whose joint surface corresponds to only about a third of the humerus head. This anatomical structure of the shoulder joint enables very extensive mobility of the shoulder and arm. These somewhat unfavorable proportions of the two joint partners are compensated for by various anatomically important structures that ensure that the shoulder joint remains stable and does not dislocate (luxated).

For example, the surface of the joint socket is made up of the so-called joint lip (Glenoid labrum) is elastically enlarged and the entire shoulder joint is encompassed by a joint capsule that stabilizes and centers the head of the humerus. The optimal freedom of movement in all spatial directions of the shoulder is only possible at the expense of the stability of the joint. This explains why of all the joints in the human body, the shoulder dislocates the most.
Causes of shoulder joint instability
A shoulder joint instability can innate be or after an accident occur. Shoulder instability is often the result of one traumatic shoulder dislocation (Dislocation) to one sudden rupture of the joint lip or the joint capsule.
The most common injury in the context of shoulder joint instability is the so-called "Bankart Lesion". This is usually through a Dislocation of the shoulder forward caused in an accident, with the joint lip in the lower area of the front edge of the socket tearing off partially or completely. Due to the Bankart lesion, the joint lip can no longer properly stabilize the shoulder joint in this area and it can easy to (further) dislocation of the shoulder come.
Symptoms of shoulder joint instability
The instability of the shoulder joint can be felt strong pain express. An instability and associated weakness in the shoulder area and the Inability to move the shoulder, are also described. It can be a Swelling in the shoulder joint occur as well Numbness and tingling sensations (Paresthesia) around the shoulder or in the Fingers.
Shoulder joint instability most commonly occurs after an accident event, mostly during a sporting activity like football or downhill skiing. It is not uncommon for the accident to initially lead to one Shoulder joint dislocation (Dislocation of the humerus head), which must be adjusted (repositioned) again. The risk of subsequent further dislocations is reduced
- the anatomical requirements
- the age of the person concerned and
- the corresponding sporting activity
certainly.
In some cases, shoulder joint instability is not preceded by an accident. Here should be a detailed diagnostics to check whether a surgical approach is required or whether conservative (non-surgical) treatment of the instability can be attempted first.
Appointment with a shoulder specialist

I would be happy to advise you!
Who am I?
My name is Carmen Heinz. I am a specialist in orthopedics and trauma surgery in the specialist team of .
The shoulder joint is one of the most complicated joints in the human body.
The treatment of the shoulder (rotator cuff, impingement syndrome, calcified shoulder (tendinosis calcarea, biceps tendon, etc.) therefore requires a lot of experience.
I treat a wide variety of shoulder diseases in a conservative way.
The aim of any therapy is treatment with full recovery without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
You can find more information about myself at Carmen Heinz.
Diagnosis of shoulder joint instability
First, an in-depth Questioning the person concerned (anamnese) regarding the discomfort caused by the shoulder joint instability. To secure the diagnosis, the clinical examination of the shoulder joint as well imaging methods necessary. In this way, valuable information about pathological changes in the shoulder joint and the associated soft tissue structures can be collected.
Standard is one X-ray of the shoulder joint, sometimes also one Magnetic resonance imaging of the shoulder (MRI, magnetic resonance scan of the shoulder joint) be revealing. If an operation to treat shoulder joint instability is to be performed, some laboratory tests are usually required beforehand, and rarely one EKG (Electrocardiogram) and a Chest x-ray be performed.
The clinical picture of shoulder joint instability can vary depending on
- extent
- frequency
- Severity and
- direction
be divided into different categories.
First of all, a Dislocation distinguished from subluxation be there with a complete dislocation (dislocation) there is no longer any detectable contact between the joint surfaces. Furthermore, one differentiates depending on the cause traumatic (with accident) from one atraumatic (without accident event) shoulder joint instability. Most acute dislocationsn take place forward (anterior) or anterior-inferior, which is very rare Direction of dislocation backwards (dorsal).
Therapy of shoulder joint instability
Treatment of shoulder joint instability can essentially be based on two different types respectively:
1. Conservative therapy
A dislocated shoulder should as soon as possible adjusted again (repositioned) become. Before that, one should X-ray control be carried out to exclude bony injuries. The reduction can, if necessary, in a Short anesthesia be performed. If the shoulder has been dislocated before, it may be possible to reduce it without anesthesia.
In some cases, conservative (non-surgical) treatment may also be possible, taking into account the individual anatomical causes of the shoulder instability. This will cause pain appropriate pain reliever medication and after the reduction, the Shoulder immobilized for a short time (e.g. in a Gilchrist Association). Following is a intensive training of the muscles (especially the back muscles) under physiotherapy instructions makes sense.
2. Operative therapy
Surgical therapy for shoulder instability aims at the present Correct injuryin order to restore the normal anatomy as precisely as possible. The shoulder instability surgery is done in most cases arthroscopic carried out, that is, as part of a Jointoscopy. This surgical technique is minimally invasivebecause usually only two to three small incisions in the skin about one centimeter in length are required.
Only in a great way rare cases can a open surgical procedure required be, for example, if bony chippings are caused by a shoulder dislocation and free in the joint space "swim around". In an arthroscopic procedure, optics with a camera system and corresponding special instruments are inserted through the small openings in the shoulder joint. In this way, the existing damage to the shoulder joint can be repaired, often the torn off capsule or the torn joint lip using a suture anchor reattached to the bone. These threads are bioabsorbable implantswhich means that they are dissolve after a certain time and don't have to be pulled. After this time, the anatomical structure has healed again.
Follow-up treatment after the operation
Immediately after the operation, the affected person will receive a Shoulder splint (Orthosis) created the only one very limited mobility of the shoulder joint. Through the protection a Stabilization and scarring process use, which usually leads to a stable shoulder again. There is a temporary Limitation of mobility in the shoulder, especially under Avoidance of splaying and external rotation movements (this could dislocate the shoulder again). The chances of success with surgical treatment of shoulder joint instability are very good over 95 percent stability of the shoulder joint can be achieved again. The prerequisite for this is a optimal aftercare according to the recommendations of the attending physician or therapist.