Therapy of stomach cancer
All information given here is only of a general nature, tumor therapy always belongs in the hands of an experienced oncologist!
Synonyms
Medical: gastric cancer
Gastric tumor, gastric Ca, gastric adenocarcinoma, cardiac tumor
definition
Of the Gastric cancer (gastric cancer) is the fifth most common cancer in women and the fourth most common in men. The gastric carcinoma is a malignant, uncontrollably growing tumor that is caused by the cells of the Gastric mucosa descends. The causes of stomach cancer are among others Nitrosamines from food, nicotine and Helicobacter pylori discussed. In most cases, the tumor causes symptoms late, when it is already well advanced. Due to the late diagnosis, stomach cancer is often treated late, so that this type of cancer has a very poor prognosis for the patient.
Figure digestive tract
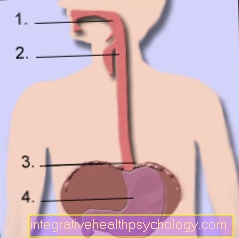
- Throat / throat
- Esophagus / esophagus
- Stomach entrance at the level of the diaphragm (diaphragm)
- Stomach (gaster)
TNM classification gastric cancer
Through the on the previously mentioned page for Diagnosis of stomach cancer the tumor stage is determined.
The tumor stage is decisive for further therapy planning. However, an exact assessment of the tumor stage is often only possible after the operation, when the tumor has been removed (resected) and it and the lymph nodes have been examined finely (histologically). There are different classifications for gastric tumors, for example according to the appearance of the tumor cells, the type of growth or the location in the Stomach.
The TNM classification is the generally recognized classification system for tumors of various types.
T stands for the tumor size and its extent in the wall layers of the organ
N stands for the number of affected lymph nodes
M. for tumor settlements (metastases) in distant organs.
Classification
T: primary tumor
TX: primary tumor cannot be assessed
T0: no evidence of primary tumor
Tis: Carcinoma in situ, tumor cell detection without invasion into the lamina propria mucosae
T1: tumor grows into the lamina propria mucosae and / or submucosa
T2: tumor grows into the muscularis propria or subserosa
T3: Tumor grows into the serosa, neighboring organs are tumor-free
T4: Growing into the neighboring organs (large intestine (Colon transversum), liver (Hepar), pancreas (pancreas), diaphragm), spleen (flushes), abdominal wall.
(The gastric wall layers are explained on the Stomach Anatomy page.)
N: lymph node involvement
NX: regional lymph nodes cannot be assessed
N0: no regional lymph node metastases present
N1: metastases in 1-6 regional lymph nodes present
N2: metastases in 7-15 regional lymph nodes
N3: metastases in more than 15 regional lymph nodes
M: distant metastases
MX: Distant metastases cannot be assessed
M0: no distant metastases present
M1: Distant metastases present
R - additional classification
R: After the operation (resection)
R0: Complete tumor removed
R1: only microscopically visible residual tumor remained.
R2: with the naked eye (macroscopic) residual tumor remained
therapy
The treatment of the patient requires intensive collaboration between the specialist in surgery, internal medicine, radiation therapists and pain therapists.
In therapy, the TNM classification is used as an essential aid to decision-making. There are corresponding therapy guidelines for each tumor stage. So one can describe three treatment goals that are considered depending on the stage.
Operational approach
The patient's only chance of cure is to radically remove the tumor, i. to operate out as a whole (R0 resection), which is only possible in about 30% of patients. Since gastric cancer is usually only recognized late and thus treated, a total stomach removal (gastrectomy) often has to be performed, which is always accompanied by a generous lymph node removal.
Often the large (greater omentum) and small mesh (minus omentum) and the spleen (splenes) are also removed (resected). Depending on the location of the tumor, a distinction is made between different surgical techniques.
The surgeon has various options at his disposal to restore the continuity of the gastrointestinal tract and to reconstruct a connection between the remaining stomach and the subsequent intestine (anostomosis).
- Antral carcinoma
In the case of a tumor located in the area of the exit of the stomach, part of the stomach can be preserved if the tumor spreads. A 2/3 or 4/5 resection should be considered.
With diffuse growth of the tumor, a total removal of the stomach (gastrectomy) is indicated here as well. - Body carcinoma
The tumors located in the body (main part) of the stomach are treated with a radical stomach removal. - Cardiac cancer
The tumor at the entrance to the stomach is also removed by a total gastric resection. The lower esophagus is also removed.
In some patients the tumor process is very advanced, so that no more healing (curative) surgery can be performed. However, there are many different operations available that can alleviate the symptoms (palliative therapy). The focus is on operative techniques that ensure the passage of food.
Tissue diagnostics
The removed stomach tumor is examined microscopically (histologically) after the removal of the tissue. For this purpose, the tumor specimen is cut at certain points and at the resection margins. From these samples, wafer-thin sections are made, stained and assessed under the microscope. The tumor type is determined, its spread into the stomach wall is assessed and the lymph nodes with removed lymph nodes are examined for tumor involvement. In order to completely rule out lymph node involvement, the pathologist must examine at least 6 lymph nodes. Only after the tissue findings can the tumor be clearly described according to the TNM classification.
Radiation therapy (radiotherapy)
Radiation therapy is used for this type of tumor when the tumor is inoperable and does not respond to chemotherapy.
Stomach cancer cannot be cured with radiation therapy.
Chemotherapy (drug therapy)
Since stomach cancer is usually adenocarcinoma (see above), it usually does not respond well to chemotherapy. As with radiation therapy, chemotherapy is used as a palliative therapy when there is no longer any possibility of surgery. Sometimes chemotherapy is also used to reduce the size of the tumor and make it operable (neoadjuvant therapy).
Stent insert
If the food pathways are severely narrowed by the tumor, the patient must be fed with aids. In order to keep the food passage open, a plastic tube (tube) or a tubular wire frame (stent) must occasionally be implanted. These surgical procedures can usually be performed in a minimally invasive manner during a gastroscopy.
Laser therapy
Laser therapy can be used as an alternative to a tube or stent. Here, the parts of the tumor that obstruct the passage of food are vaporized by the laser, reducing the extent of the esophagus or stomach narrowing. Unfortunately, the tumor often grows back from the layers below, so that the treatment sometimes has to be repeated after 7-14 days.
Feeding fistula / percutaneous endoscopic gastrostomy (PEG)
When other therapy options fail to keep the food passage open, a tube called a feeding tube (PEG) can be placed directly through the skin into the stomach. This method of treatment is a small surgical procedure. Under endoscopic control, a hollow needle (cannula) is first pushed through the skin and into the stomach in order to insert a plastic tube over it as a permanent connection to the stomach. In contrast to a gastric tube placed through the nose, the PEG offers many advantages for the patient:
The patient can feed himself food ("astronaut food") through this tube. The tube clogs less easily than the nasogastric tube and you can feed more food at once. Another important point for the patient, however, is aesthetics, as the tube disappears under clothing, invisible to others.












.jpg)