Duodenum
Location and course
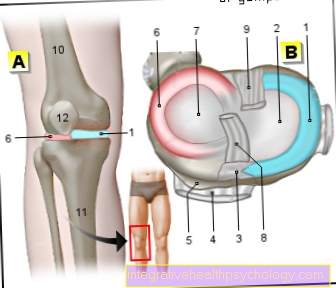
The duodenum (Duodenum) is part of the small intestine and forms the connection between the stomach and the jejunum (Jejunum). It has a length of approximately 30 cm and is anatomically divided into 4 different sections depending on its course.

Illustration of the duodenum

- Duodenum -
Duodenum - Pancreas -
Pancreas - Small intestine -
Intestine tenue - Jejunum -
Jejunum - Right kidney -
Ren dexter - Gallbladder - Vesica biliaris
- Liver - Hepar
- Stomach - Guest
- Duodenum
descending part -
Duodenum pars
descending - Duodenum
upper part -
Duodenum pars
superior - Gastric gate muscle -
Pyloric sphincter muscle - Section of the stomach near the gatekeeper -
Gaster pars pylorica - Large duodenal papilla -
Major duodenal papilla - Duodenum
lower part -
Duodenum pars
inferior - Duodenum
ascending part -
Duodenum pars
ascending - Duodenal
Jejunum junction -
Duodenojejunal flexure - Jejunum -Jejunum
You can find an overview of all Dr-Gumpert images at: medical illustrations
After leaving the gastric porter, the chyme reaches (Pylorus) first the upper part of the duodenum (Pars superior). This section is made up of the right lobe of the liver and the front of the gallbladder (ventral) covered.
On the back (dorsal) lies both the Bile duct (Common bile duct) as well as part of the portal vein.
An anatomical peculiarity is that the upper part of the duodenum is the only one inside the peritoneum (peritoneum) lies (intraperitoneal location).
The remaining sections of the duodenum are all fused with the posterior abdominal wall; their position is referred to as secondary retroperitoneal.
The pars superior duodeni is particularly prone to Duodenal ulcers (Ulci), which can be caused by the sour food pulp from the stomach.
Adjacent to the upper part of the duodenum is the clinically important descending part (Pars descendens). This importance is mainly due to the fact that on the one hand the Bile duct and on the other hand the Duct of the pancreas (Pancreatic duct) via a common opening (Major duodenal papilla) flow.
Get in this way Digestive enzymes the pancreas and bile acids of the liver in the intestines and ensure a functioning digestion there. In addition, the acidic food pulp is neutralized by the basic components of the secretions.
The third section of the duodenum forms the horizontal part (Pars horizontalis). It is located approximately at the level of the third lumbar vertebra and pulls in front of the spine to the left half of the body.
There the horizontal part flows into the last section of the duodenum, namely the so-called ascending part (Pars ascendens). As its name suggests, this fourth segment of the duodenum takes a course towards the diaphragm, i.e. upwards (cranial), on.
At the level of the first lumbar vertebra, the ascending part penetrates the abdominal cavity (after intraperitoneally) and goes into the subsequent section of the small intestine, the Jejunum, over.
If you now look at the course of the individual sections of the duodenum, it is roughly similar to the letter C.
This is interesting in that the Head of the pancreas exactly fits into this bulge. This close positional relationship is also the reason why Pancreatic cancer often grows into the duodenum and damages it.
If there is a crack (perforation) of the duodenum, for example due to an injury to the abdomen or a Intestinal obstruction (Ileus) chyme can enter the abdominal cavity and become life-threatening inflammation or Blood poisoning (sepsis) to lead. An instant one surgery is essential for survival in this case.
Illustration small intestine

- Small intestine -
Intestine tenue - Duodenum, upper part -
Duodenum, pars superior - Duodenal
Jejunum junction -
Duodenojejunal flexure - Jejunum (1.5 m) -
Jejunum - Ileum (2.0 m) -
Ileum - End part of the ileum -
Ileum, pars terminalis - Colon -
Intestinum crassum - Rectum - Rectum
- Stomach - Guest
- Liver - Hepar
- Gallbladder -
Vesica biliaris - Spleen - Sink
- Esophagus -
Esophagus
You can find an overview of all Dr-Gumpert images at: medical illustrations
Microscopic structure
The different layers of the duodenum in cross section correspond to those of the rest of the digestive tract.
From the outside, the duodenum is from connective tissue (Tunica adventitia) which surrounds both Blood-, as well as Lymphatic vessels contains.
It borders a Muscle layer, the so-called Tunica muscularis. It contains an outer longitudinal and an inner circular muscle layer that the peristalsis serve.
There is one between the two muscle layers Nerve plexus (Myenteric plexus), which innervates the smooth muscles and the own nervous system belonging to the intestine (enteric nervous system).
Another plexus of nerves is found in the one following the tunica muscularis Tela submucosa. This is the Submucosal plexus, which is embedded in the loose connective tissue of the tela submucosa.
The innermost layer is one Mucous membrane (Tunica mucosa), which can still be divided into three different sub-layers. The interior of the duodenum is made up of the Lamina epithelialis mucosae lined. This is followed by a thin layer connective tissue (Lamina propria mucosae), which in turn has its own Muscle layer of the mucous membrane (Lamina muscularis mucosae).
But what is the difference between the structure of the duodenum and that of the rest of the digestive tract?
To Differential diagnosis There are basically two different features. On the one hand, there are special ones in the tela submucosa Brunner's glands, the only in the duodenum occur and a viscous secretion submit.
On the other hand, it shows Mucous membrane of the duodenum macroscopically abnormal Protrusionsthat one as Plicae circulares designated. These serve together with Villi and Crypts, which consist of the lamina epithelialis mucosae and the lamina propria mucosae, the Surface enlargement of the lumen of the duodenum. This makes it very efficient Absorption the food particles guaranteed.
Blood supply
The Blood supply of the duodenum takes place over two large branches of the main artery (aorta).
A rises approximately at the level of the twelfth thoracic vertebra Vascular stem from the aorta (Celiac trunk), which is instrumental in the care from spleen, liver, pancreas and stomach is involved. A branch of the celiac trunk, namely the Common hepatic artery, also delivers a vessel (Gastroduodenal artery). This artery mainly supplies the upper sections of the duodenum with blood.
The parts below of the duodenum receive their blood supply via the upper mesenteric artery (Superior mesenteric artery). It arises directly from the abdominal aorta at the level of the first lumbar vertebra. The arteria mesenterica superior also represents next to the duodenum Inflows to the entire small intestine, as well as for Large intestine up to the left colon flexure.
Function of the duodenum
The small intestine is divided into three areas. The first section that goes directly to the stomach is the Duodenum or duodenum called. It got its name because of its length of about 12 finger widths.
After the stomach has mainly mechanically chopped up the food and with the help of stomach acid has almost completely freed the food pulp of bacteria and other microorganisms, it reaches the duodenum. There the chyme is first neutralized, because otherwise it would damage the mucous membranes of the intestines due to its low pH value. A corridor leads to this, the Pancreatic duct, into the duodenum, through which an alkaline secretion is released from the pancreas. The bile duct also joins this duct (Common bile duct), which leads the bile into the duodenum.
The bile is produced in the liver and then stored in the gallbladder until it is needed in the duodenum to digest fats and fat-soluble vitamins. In addition, cells in the lining of the duodenum form enzymes that initiate the digestion of the individual nutrients. Finally, water is added to the chyme here.
In the duodenum it is found actual digestion the food, i.e. the breakdown of the nutrients it contains. Only later, in the back two sections of the small intestine, are the nutrients actually absorbed into the body.
Enzymes of the duodenum
Enzymes are special Proteins, the Catalyze reactions. This means that they accelerate the process and thus reduce the energy required for the reaction. In the duodenum, enzymes are added to the food. There they then split the nutrients they contain into their smallest units so that they can be absorbed by the intestine.
Each individual class of nutrients has its own highly specific enzymes. Proteins are broken down by so-called proteinases, for example trypsin, fats by lipases and the various types of sugar by amylase, lactase, isomaltase and maltase-glucoamylase. The product is amino acids in the case of proteins and simple sugars such as glucose and fructose in the case of the breakdown of the multiple sugars. Individual fatty acids are formed when fats are broken down.
This breakdown of our food represents the actual process of digestion and is necessary because transporters across the cell membranes are only available for the small nutrient components. The amylases and lipases come from the secretion of the pancreas. The other enzymes come with the food pulp from the mouth and stomach into the duodenum and some of them are produced directly by cells of the duodenum.
Diseases

The most common disease of the duodenum is duodenal ulcer (Duodenal ulcer). The lesion is usually just after it exits the stomach (Pylorus) and can have various causes.
These include stress, a bacterial infection (Helicobacter pylori), over-acidification of the intestine, for example due to stomach acid, or long-term use of anti-inflammatory drugs such as aspirin. A duodenal ulcer initially manifests itself as severe pain in the middle upper abdomen and severe nausea.
Irregular bowel movements and unwanted weight loss can also be consequences of a duodenal ulcer. If the course is particularly severe, it can lead to profuse bleeding of the upper digestive tract or even to a tear in the duodenum.
In such a situation, the ulcer should be treated surgically. In some cases, however, the ulcer is completely symptom-free and was discovered more by chance during routine examinations.
In addition to antibiotics, so-called proton pump inhibitors such as omeprazole and pantoprazole are also available for drug treatment. These inhibit the gastric acid produnction and are intended to protect against further acidification of the duodenum. 90% of patients are freed from a duodenal ulcer after such therapy.
Inflammation of the duodenum
In the area of the duodenum, inflammation, i.e. strong immunological reactions, can occur due to various causes. On the one hand, an Einflammation of the stomach (Gastritis) spread to the duodenum. The ingestion of Medication that irritate the mucous membrane and make it sensitive to the smallest injuries and an infestation with disease-causing substances. Similar to cancer, inflammatory cells can also migrate from the pancreas into the duodenum or even infiltrate and damage the intestinal wall from outside.
Inflammation does not always have to manifest itself through symptoms, but abdominal pain, fatigue, nausea and anemia can occur. Anemia occurs because the area of inflammation increases blood flow while the vessels can become more fragile. Smallest amounts of blood then leak out and are excreted in the stool.
To be able to secure the diagnosis, must Tissue samples removed endoscopically from the duodenum and examined by a pathologist.
The treatment arises from the cause. So if there is a bacterial inflammation, you can Antibiotics are given. In addition, drugs that promote inflammation should be avoided. These drugs include the non-steroidal anti-inflammatory drugs such as aspirin (ASA).
However, duodenitis can also take a chronic, i.e. permanent form. Then one speaks of one inflammatory bowel disease. Such a chronic inflammation is Crohn's disease, the cause of which is still unknown. It occurs very rarely in the duodenum and is mostly found in the ileum. The symptoms are similar to those of normal inflammation. On the other hand, due to the as yet unknown cause, the therapy is particularly aimed at eliminating complications such as additional bacterial infections in the area. The disease progresses in relapses, so strong anti-inflammatory drugs such as glucocorticoids can be given in acute situations.
Duodenal cancer
Fortunately, duodenal cancer is pronounced Rare. Much more common Colon cancer and rectum on. This has various causes, but not all of them have been clarified yet. On the one hand, the time aspect plays a role, because the food pulp is only briefly in the small intestine and especially in the duodenum, while it remains in the colon for up to days. As a result, the contact time of pollutants and potentially cancer-causing substances in food with the mucous membrane of the large intestine is much longer. And the longer this time, the more likely it is that the substances will actually be absorbed into the body.
Another possible explanation is the function of the duodenum. As already mentioned, mainly enzymes and fluids are released from the cells of the mucous membrane. So there are no cellular mechanisms available that could absorb substances into the cells in the first place. It is completely different in the subsequent sections of the small intestine. There special transporters can be found in the cell membranes that enable the absorption of food components and thus also possible pollutants. Once cancer cells appear in the duodenum, they usually originate from a tumor located in the pancreas. Since these two organs are very close to each other, it is very easy for cancer cells to spread from the pancreas into the duodenum.
Duodenal ulcer
Contrasted with duodenal cancer Ulcers in this area of the small intestine much more often on and will too Duodenal ulcer called.
Ulcers are defects in the mucous membrane that can reach into the deepest layers. As a result of an infection or circulatory disorder, an area is no longer adequately supplied with blood and immune cells, as a result of which it slowly loses its function and ultimately dies. There are people who, because of their genes, have an increased risk of developing ulcers.
Usually the cause lies in the ingestion of Medicationsuch as aspirin, which prevent stomach mucus from building up. As a result, the stomach and the subsequent duodenum are no longer adequately protected against the very acidic gastric juice and are attacked by the acid. These superficial injuries then spread into deeper and deeper layers of the multi-layered intestinal wall and thus cause the ulcers.
In many cases it can also Bacterium Helicobacter pylori cause one gastritis, an inflammation of the stomach. This can then develop into an ulcer.
Probably the most common symptom are stomach painfollowed by the symptoms of a anemiahow fatigue and pallor. The anemia is caused by a small, albeit constant, loss of blood from the ulcer.