Scapholunal dissociation / SLD
Synonyms in a broader sense
Scapholunal dissociation, scaphoid dislocation, wrist ligament injury, distal radius fracture, hand injury
definition
At a scapholunal dissociation / SLD the ligaments in the carpal area between the Scaphoid (Os scaphoideum, formerly Os naviculare) and the Moon leg (Os lunatum).
root cause
Scapholunal dissociation / SLD is the second most common accident-related carpal disease after the scaphoid fracture. Scapholunal dissociation / SLD can only arise as a result of an accident and can occur in combination with a distal radius fracture.
Typical accidents are a fall on the outstretched wrist.

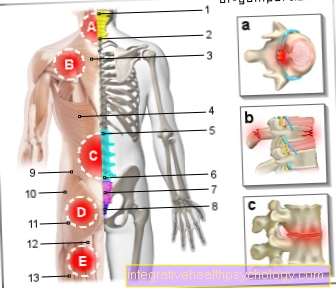
Grade 3: Complete rupture of the ligamentous apparatus between the scaphoid bone and the lunar bone with visible malalignment and divergence of the lunate bone (Os lunatum) and the scaphoid bone (Os scaphoideum, formerly Os naviculare). Compare the healthy wrist below, there is no gap between the navicular bone (1st) and the lunar bone (2nd).
Symptoms
Typical symptoms of scapholunal dissociation / SLD are the pain in the wrist area, and most importantly Pain in the navicular bone. Which cannot be distinguished from a scaphoid fracture or wrist fracture without further examination by the doctor.
So-called click noises can sometimes be heard and snapping phenomena can be seen and felt, which are caused by cartilage damage.
The mobility of the wrist is significantly restricted by the lack of movement of the first row of carpal roots.
Due to the incorrect position of the carpal bones Scaphoid (Os scaphoideum) and Moon leg (Os lunatum) the strength in the wrist is reduced.
If this injury persists for a longer period of time, a swelling can be felt over the back of the hand, which is caused by an overgrowth of the joint mucous membrane (synovitis).
Classification
Scapholunal dissociations are classified into three degrees of severity.
Grade 1: partial tear of the ligamentous apparatus between the scaphoid and the lunar bone without any detectable instability
Grade 2: partial tear of the ligamentous apparatus between the scaphoid and the lunar bone with provocable instability
X-ray wrist

- Scaphoid bone (scaphoid bone)
- Moon bone (os lunatum)
- Pea bone (os pisiforme)
- Triangular bone (os triquetum)
- Hook bone (os hamatum)
- Head bone (os capitatum)
- small polygonal bone (os trapezoidum)
- large polygonal bone (os trapezium)
diagnosis
The first step is a clinical examination of the wrist. There should be specific tests to prove (postponement test according to Watson) whether an SLD can be diagnosed with this, however, appears questionable.
As a further measure, an x-ray of the wrist will be carried out in two planes. Third degree scapholunal dissociation / SLD can result from the extended distance can be diagnosed between the navicular bone and the moon bone (> 2 mm). To secure the diagnosis, the opposite side can also be x-rayed in order to rule out system-related variants.
First and second degree injuries can only be done with the MRI (magnetic resonance imaging) be detected.
therapy
Conservative and surgical methods are available for treating scapholunal dissociation.
Conservative therapy is used for minor injuries. It involves repositioning the bones in their anatomical position with a subsequent 6-week immobilization in a cast or a wrist bandage. During this time, the SL ligament should grow back together and heal stably. Painkillers can also be taken during this time as needed.
Both minimally invasive and open operations are available for surgical treatment. With the joint endoscopy, small pieces of cartilage and ligaments that cause discomfort in the wrist can be removed. Attempts can be made to sew the SL tape within the first few weeks after the injury. Ligament surgery, ligament transplants or other procedures can then be performed to restore the anatomical conditions. However, these operations promise only a low success rate. As the last therapeutic method in the case of beginning or advanced cartilage wear, stiffening at the wrist comes into question. This slightly restricts mobility in the joint, but the wrist remains painless and stable.
Read more about the topic here: Therapy for scapholunal dissociation
Healing time
Both conservative and surgical therapy take several weeks to heal.
In conservative therapy, the wrist must be immobilized and immobilized for about 6 weeks using a cast or bandage. There is also a 6-week grace period after surgical suturing of the SL ligament or the treatment of other accompanying injuries. Even after that, the load on the wrist should only be increased slowly. Complete mobility can only be achieved slowly through passive and active movement exercises. As a rule, the wrist reaches its complete stability and mobility after about 12 weeks.
forecast
The prognosis of scapholunal dissociation cannot be given in general terms, but must be made dependent on the respective extent and the accompanying injuries. It is important to notice the injury early on. If the diagnosis is made immediately, the injury can heal in a stable and sustainable manner within 6 weeks with conservative therapy and consistent immobilization.
Surgical sutures of the torn ligament are also possible within the first month. Subsequent surgical therapies are difficult to restore the anatomy. In many cases, the joint has to be stabilized in other ways, in some cases even through partial stiffening. The most important goal is to achieve the best possible pain-free movement in the joint. This is usually possible after therapy.
When do you need an operation?
Scapholunal dissociation can take on different dimensions and thus be associated with different complaints and consequences. The disease can be divided into 3 grades. In all cases there is damage to the scapholunal ligament, which allows the lunar bone and the navicular bone to slide apart.
If there is only a slight displacement of the bones, a so-called "dislocation", conservative therapy may be sufficient.
From grade 2 of the disease, however, there are additional shifts, malpositions, instabilities, cartilage and bone damage. In these cases, surgical treatments are necessary to treat the injured structures and to fix the SL ligament. Various surgical procedures are available for this, in some cases minimally invasive joint endoscopies are also possible.