Kneecap
Synonyms
Kneecap fracture, patellar fracture, pendulum tendon, patellar tendon, patellar tendon, chondropathia patellae, retropatellar arthrosis, patellar dislocation, patellar dislocation
Medical: patella
English: patella
Figure kneecap
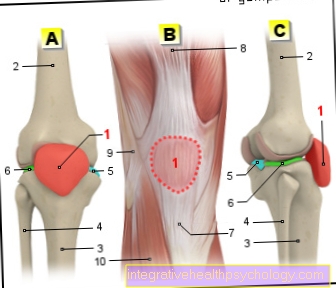
- Kneecap -
patella - Femur -
Femur - Shin -
Tibia - Fibula -
Fibula - Inner meniscus -
Meniscus medialis - Outer meniscus -
Lateral meniscus - Kneecap ligament -
Ligamentum patellae - Hamstring muscle -
Rectus femoris muscle - Iliac-tibial tendon -
Iliotibial band - Tibia anterior muscle -
Tibialis anterior muscle
You can find an overview of all Dr-Gumpert images at: medical illustrations
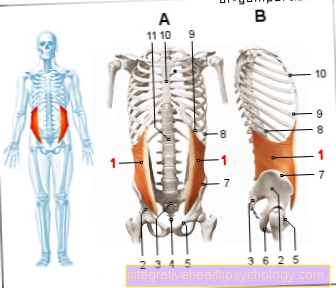
anatomy
So that the front Thigh muscles can transfer the force favorably to the lower leg when the knee joint is bent, this is necessary Knee joint a spacer. This spacer is the Kneecap / patellathat works as a kind of force diverter.
At the top of the kneecap, the large anterior thigh muscles (Quadriceps femoris muscle) with a tendon end directly.
On the underside of the kneecap, the kneecap tendon / patellar tendon (ligamentum patella) pulls towards the front of the tibia (Tibia). There it attaches to a small protrusion of bone (apophysis = tibial tuberosity). Actually, the patellar tendon is not a type of vision, since by definition a muscle must be involved in a tendon. However, the kneecap tendon connects the kneecap (bone) with the shin (tibia). This is why the patellar tendon is known medically as a ligament.
So that the kneecap can transmit the force directly, there is a slide channel between the two heads of the thighs, in which the kneecap / patella can slide about 5 - 10 cm when bending and stretching.
The back surface of the kneecap is covered with a thick layer of cartilage (hyaline cartilage) overdrawn. Corresponding to the sliding channel of the thigh, the rear surface is a longitudinal one First with a smaller inner and a larger outer outside (medial and lateral facet the patella). Both sliding surfaces are usually at an angle of 120 - 140 ° to each other (ridge angle = patella opening angle).
The size and the angle of position of the two facets is important, since uniform power transmission and low wear are only possible with an ideal size.
Patellar dadysplasia

Plant-related shape variants
- normal kneecap
- Dysplastic kneecap
- Dysplastic kneecap with lateralization
- Retropatellar cartilage damage
function
The kneecap transfers the force of the front thigh muscles to the shinbone via the knee joint. The kneecap / patella functions as a physical force diverter (hypomochlion).
When bending and stretching to the maximum, the kneecap can slide approx. 10 cm in the sliding groove of the thigh bone.
Kneecap dislocation
In the Kneecap dislocation (Patellar luxation) the kneecap has jumped out of its predetermined path of the thigh. If the kneecap has jumped out, the capsular ligaments always tear.
Are risk factors for a dislocation of the kneecap (patellar dislocation) Knock knees, a loose ligament apparatus (hyperlax) and a raised kneecap.
The kneecap has practically always jumped out of its slideway. A kneecap that pops out once again carries the risk of popping out again.
Further information is available under our topic: Kneecap dislocation
Appointment with a knee specialist?

I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Diseases of the kneecap
Retropatellar arthrosis
The most common disease of the kneecap (patella) is osteoarthritis of the kneecap (retropatellar arthrosis).
There are many causes of kneecap arthrosis. Possible causes can be poor cartilage quality due to the anal area, incorrect positioning of the kneecap (facet hypoplasia, incorrect ridge angle), knock knees, bow legs, patellar lateralization (the kneecap slides too far outside in the slide channel, etc.).
For more information, see: Retropatellar osteoarthritis

Stages of osteoarthritis
(Chondromalacia according to Outerbridge) from top to bottom:
- Grade 1 chondromalacia
- Grade 2 chondromalacia
- Grade 3 chondromalacia
- Grade 4 chondromalacia
Chondropathia patellae
As Chondropathia patellae is a mostly harmless but often very painful strain on the kneecap of children and adolescents. Express this Pain behind the kneecap when climbing stairs and taking a deep squat.
In most cases this pain goes away by the age of 25-30. However, it must be ensured that there is no cause of illness behind the complaints.
Osgood-Schlatter disease
The Osgood-Schlatter disease is defined as a painful one irritation the starting point of the tendon of the Kneecap (= Patellar tendon). The attachment point is at the front Shin. With juvenile osteochondrosis there is also the risk that Pieces of bone detach from the shin and thereby die, become necrotic. The dead bone part is also called aseptic osteonecrosis designated. In this context, aseptic means that it was not caused by an infection.
At the Osgood-Schlatter disease younger people are mainly affected, often between the ages 10 and 14 years. It could also be observed that boys four times suffer from Osgood-Schlatter disease more often than girls. The disease can only be one both knee infested. It is believed that with excessive Sports (especially to jog or Leap) very small Injuries that are the cause of the disease.
Read more on this topic under Osgood-Schlatter's disease bandage
Patellar lateralization
In the Patellar lateralization the kneecap runs too far out in the gliding groove of the thigh. This results in an asymmetrical load on the kneecap (the outside is more stressed).
The cause is usually a misalignment of the kneecap and / or the sliding bearing in combination with a weakness of the inner anterior thigh muscles (musculus vastus medialis).
Prepatellar bursitis
Large sliding surfaces are necessary to allow the kneecap to slide. There are two bursa on the knee joint that enable this gliding. The so-called is located directly in front of the kneecap Prepatellar bursawhich can ignite with small skin injuries, sometimes for no apparent cause.
An inflammation of this bursa (Prepatellar bursitis) can have far-reaching consequences. In the case of pronounced inflammation there is a risk of knee infection (knee joint empyema) or Blood poisoning. Therefore, the bursa has to be removed if the infection is severe.
Sindling Larsen's disease
Of the Sindling-Larsen disease is a rare disease of growing age (usually 10-14 years of age). This is a circulatory disorder of the lower kneecap pole. In most cases, this disease heals without consequences, even without therapy with sports leave.
Patella bipartia
In some cases the kneecap is doubled or the connection between different bone cores is missing. In most cases there is an additional bone (patella bipartita) in the upper outer quadrant of the kneecap, which in itself has no disease value.
A total of up to six bone parts can occur. However, as the number of fragments increases, the risk of premature cartilage wear behind the kneecap increases.
Read more on the subject at: Bipartite patella
Patellar tip syndrome
Athletes often suffer from one Patellar tip syndrome. It is a chronic, painful, degenerative overuse disease of the kneecap extensor apparatus at the bone / tendon junction of the kneecap tip.
Further information is available under our topic: Patellar tip syndrome
Kneecap jumped out

When the kneecap (patella) pops out of its normal position, this is also called Patellar luxation designated.
Some risk factors can promote patellar dislocation. Above all, this includes one undeveloped patella, the so-called Patellar dysplasia.
In this case, the kneecap is often too small and is not sufficiently fixed by the ligamentous apparatus of the knee. This allows it to slip out of its holder quickly.
However, such a patellar dysplasia usually already falls before the age of 20 for the first time due to a dislocation and the dislocations keep happening.
Other favorable factors are an incorrect development of the ligamentous apparatus of the knee, Knock knees (Genu valgum), a weak connective tissue, as well as muscular imbalances between the upper and lower legs.
All of these factors can reduce the fixation of the kneecap so that it can dislocate.
Accidents are another cause of patellar dislocation.
Usually it is one Twisting of the knee as part of a sports injury.
The kneecap usually slips to the outside of the knee. Women are affected slightly more often than men. Overall, the kneecap slipping is very painful.
Diagnostically, a patellar dislocation is usually visible from the outside at first glance. In addition, there is often a Joint effusionthat can be bloody. In most cases, the kneecap then automatically returns to its starting position (Reduction).
Nevertheless, due to the dislocation Ligament or cartilage damage remain behind who require a medical evaluation.
If the kneecap has not slipped back into its normal position by itself, it must be medically adjusted again become.
The knee is slowly extended and the kneecap is held firmly with one hand so that it does not jump back too suddenly.
It can then be slowly returned to its normal position.
In this way, ligament and cartilage injuries are avoided. Followed by a X-ray of the knee to check the position of the patella.
Any bone damage can also be seen on the X-ray.
If the patella keeps slipping out of its position, for example due to congenital patellar dysplasia, a operative therapy which should prevent the recurrent dislocations in the future.
Kneecap loose
If the kneecap is loose and often slips out of position (Patellar luxation), it is usually due to someone Ligament weakness, one Malformation of the kneecap per se (Patellar dysplasia) or one Malformation of the plain bearing the patella (Trochlear dysplasia).
The patella is fixed by the tendon of the Quadriceps muscle on the front of the thigh, which is used to straighten the lower leg.
In addition, it is also supported by the remaining Ligament structures of the knee joint stabilized.
So it can slide on the cartilaginous surface of the trochlea, which is formed from the ends of the upper and lower leg bones.
If the shape of the kneecap is not exactly congruent to its sliding bearing, an imbalance arises which leads to a Loosening of the kneecap leads in its holder. This makes her more flexible in her position.
The same applies to an unstable ligamentous system that does not adequately fix the kneecap. This also results in a Hypermobility of the patella.
In the case of a muscular imbalance, it is also possible that the kneecap is not optimally secured in its sliding bearing. A knee misalignment, for example one, can also have a beneficial effect X-leg position.
Young girls are particularly affected by a loose kneecap.
Bruised kneecap

A bruise of the kneecap is also called Knee contusion and usually arises from a sports accident or a fall.
There is a strong force acting on the kneecap, which is briefly strongly compressed with the surrounding tissue.
This does not result in a major injury to the skin, but it can Blood and lymph vessels be damaged in the kneecap area and the kneecap itself can also be damaged.
The vascular injury leads to it Bleeding into the tissue. From the outside, the bruise is as red-bluish discoloration of the skin and Soft tissue swelling visible.
In addition, the joint area is mostly overheated and reddened.
The effusion can cause it to severe pain and one Function restriction of the knee joint. Especially bending the knee (for example when climbing stairs) is perceived as painful.
As an immediate measure, it is advisable to immediately stop any strain on the affected knee in order not to worsen the symptoms.
The leg should also be raised as high as possible, as the hydrostatic pressure when standing can worsen the swelling.
The knee should be best with Ice chilled as it constricts the blood vessels and stops bleeding more quickly. The pain can also be relieved in this way.
Ultimately, a slight pressure from the outside can contain the swelling (for example through an applied bandage). It is essential to ensure that the bandage is not applied too tightly so as not to cut off the blood supply.
If the pain is very strong, so can pain relievers or medication come into use. In the case of very pronounced joint effusions, a puncture and suction of the fluid can have a relieving effect.
If the kneecap is bruised, it is always advisable to see a doctor. This can clarify through a detailed examination of the knee whether important structures of the knee (ligaments) or the kneecap itself have not been injured.
Kneecap slipped
If the kneecap slips, it is often caused by a congenital predisposition in the form of a Patellar dysplasia.
In this case it is Kneecap malformed. So it is either too small or has a shape that is not congruent to its plain bearing.
This reduces its guidance on the knee joint and it can slip more quickly.
Movements that predispose to it are particular rapid turning movements in the knee. Accordingly, the kneecap slips most frequently as part of a sports injury.
Loose ligaments in the knee area also increase the risk that the kneecap will slip out of position.
Usually it is made up of the tight ligament apparatus Inside- and Outer bands, as well as the tendon of the Quadriceps muscle sufficiently fixed. If this is not the case, it can slip. Due to the instability it can also Cartilage damage occur in the knee joint, which are usually noticeable as pain in the front knee area.
The instability is treated therapeutically in particular by reconstructing the ligamentous apparatus so that the kneecap is better fixed.
In some cases further stabilizing measures are necessary.
If the patellar instability only occurs during growth, it is often necessary to wait first, as the problem has often resolved itself by the end of the growth phase.
If not, there can be one here too operative therapy be considered.
Kneecap jumps

If the kneecap rests resiliently on the knee joint, can be moved downwards by applying pressure and then jumps up again, then the phenomenon of "dancing patella" in front.
This is a sure sign for you Joint effusion and is tested by doctors as soon as a knee joint effusion is suspected.
To do this, the leg is stretched out and the recess directly above the knee joint is stroked down with one hand.
Since there is a Bursa that can absorb relevant amounts of liquid, this should be expressed in this way. The fluid then collects below the kneecap.
Then - with further pressure exerted on the recess - the kneecap is pressed.
In the case of a joint effusion, the kneecap can now be pushed in resiliently towards the knee joint and jumps up again when you let go, as it is buoyed by the liquid level. This jumping of the kneecap is called "dancing patella" designated.
If the kneecap jumps out of its anatomically correct position during sport, for example, without any joint effusion, it is a patellar dislocation, which is usually caused either by a malformation of the kneecap, a weak ligamentous system or a muscular imbalance.
Broken kneecap
When the kneecap breaks, this is medically called Patellar fracture designated.
Usually this happens as part of a Fall or one direct violence on the knee.
Typical symptoms of a patellar fracture are a knee that can no longer be straightened and that can no longer be loaded, as well as a significant swelling, overheat and Bruising in the knee area.
The leg can no longer be bent because the kneecap acts as an abutment for the tendon of the Quadriceps muscle serves and transfers the force from the upper to the lower leg.
In the event of a fracture, the power transmission is interrupted. Accordingly, mostly exist strong pain and a Feeling of complete instability in the knee joint.
Fractures in which the entire soft tissue is torn are less common (open fracture).
To confirm the diagnosis, a regular examination of the knee joint is performed in addition to a X-ray image made on which the fragments can be clearly seen.
In this way, the attending physician can already decide on the indicated therapy.
The fact that the kneecap is connected to strong muscles means that the fracture pieces are usually strongly pulled apart so that they do not lie next to each other, but rather dislocated in the knee joint area.
Accordingly, a broken kneecap can usually not conservative be treated but requires one operational approach.
Adequate therapy with correct restoration of the anatomical conditions is particularly important, as otherwise permanent functional restrictions of the knee joint can occur.
The incorrect position of the kneecap fragments can cause further injuries to the knee joint and lead to incorrect positions with secondary posture and consequential damage to the foot and hip.
A conservative treatment in the form of a Immobilization in a cast is only possible if the fracture has not been displaced, i.e. the fragments have remained in their correct position.
The plaster of paris is intended to prevent later displacement so that the kneecap can heal normally again.
Is a operative therapy if necessary, the fragments are fixed together and the ligamentous apparatus, which has been injured, is restored. In addition, the kneecap is x-rayed intraoperatively to check that it has been assembled correctly.
Misalignments as small as one millimeter can later lead to relevant restrictions in the function of the knee joint.
It is particularly important that the Fixation of the fragments very stable because otherwise they can be pulled apart again by the forceful pull of the thigh muscles.
If the joint surface is not restored correctly, it can easily result in a arthrosis develop that with Pain and Restriction of movement goes hand in hand.
To avoid a patellar fracture from the outset, especially when doing sports with an increased risk (Inline skating, ice skating, skateboarding, cycling) knee pad be worn.
In the event of a fall, this means that the force does not act directly on the kneecap, but is absorbed and better distributed. This can usually prevent fractures.