Chronic lymphocytic leukemia (CLL)
Synonyms in a broader sense
CLL, leukemia, white blood cancer
definition
The CLL (chronic lymphocytic leukemia) is due to a uncontrolled growth of especially mature stages of Lymphocytes (Lymph cell) precursor cells, i.e. precursors of white blood cells. These mature cells, however, are unable to Immune defense. It is mainly the so-called B lymphocytes affected, rarely the so-called T lymphocytes (5%).
Get more general information about the here white blood cells
.jpg)
frequency
Strictly speaking, the CLL is a Lymphoma and not leukemia. Nevertheless, chronic lymphocytic leukemia is the most common type of leukemia overall. Older patients are particularly affected (over 60 years of age). Although older people are often affected, children can also develop CLL.
causes
So far it is largely unknown why the disease develops. Still, some could Risk factors be associated with the disease. These include in addition to old age the patient too genetic factors and various Environmental factors, such as. chemical solvents.
Symptoms
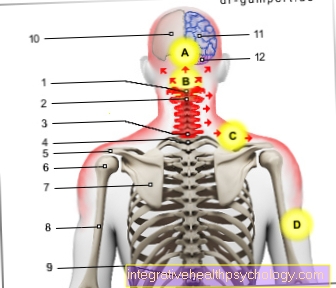
In chronic lymphocytic leukemia, lymph node enlargements occur, e.g. on the armpits or on the neck or not visible, in the abdominal cavity.
At the beginning of the disease is a Performance kink, which is typical of cancer. Motivation decreases, the patient is no longer as productive as it used to be, and patients notice significant limitations, especially when doing sport. A certain amount occurs Tendency to perspire on, especially at night. A strong unwanted one Weight loss in a short time, stronger itching and frequent infections are to be observed. Likewise is paleness a common symptom.
How do you recognize chronic lymphocytic leukemia?
The disease often goes on for a long period of time without symptoms and is therefore not uncommon late or even discovered by chance becomes.
Possible complaints can be so-called "B symptoms". These include night sweats, unwanted weight loss, and fever. However, these are quite unspecific and occur in many malignant cancers.
Often those affected notice painless enlargements of the lymph nodes. Since the leukemia cells can also affect the liver and spleen, patients often have it unspecific upper abdominal complaints, such as. a "pull" or "push".
Furthermore, CLL can become chronic itching (Pruritus) or skin rash (Urticaria) cause.
Especially in advanced stages, those affected tend to be frequent, severe Infections. For this purpose, e.g. bacterial infections, but also a pronounced herpes virus infestation count.
In some cases, painless swelling of the parotid and lacrimal glands can occur (Mikulicz syndrome).
The attending physician can usually diagnose CLL using a Blood test detect. Typical, changed blood cells can then be determined under the microscope.
Basically, however, the symptoms of the disease are unspecific, so that significantly more harmless diseases are "behind it" much more often!
diagnosis
Blood and laboratory values
In chronic lymphocytic leukemia, there are some relatively characteristic changes in blood and laboratory values.
The "Leukocytosis". This means a abnormal increase of the white blood cells. In the case of CLL, the Lymphocytes, a subspecies of white blood cells, increases. This can be explained i.a. through the extended survival time of the "malignant" leukemia cells. Put simply, these are "counted" among the lymphocytes in the blood analysis.
Often it occurs in the context of chronic lymphocytic leukemia Displacement of the normal, healthy Blood cells. As a result, a decrease in red blood cells (anemia) and platelets (Thrombocytopenia) observe.
In addition to the laboratory analysis of the blood components, the examination of the blood smear under the microscope plays a major role. Typical here is e.g. an increased number of mature, small lymphocytes or "Gumprecht umbra“.
To further characterize the CLL, there is the Immunophenotyping. During this special examination, various features on the surface of the leukemia cells are examined.
It is thus possible to form different subgroups of the disease and to optimize therapy accordingly.
Blood collection: Mostly there is an increase in white blood cells in front (Leukocytosis). In addition, parameters are also examined here that suggest an increased cell turnover (e.g. uric acid). However, an increase in white blood cells alone is not proof of CLL, since the white blood cells play an important role in the immune system and are therefore more common in inflammation or infection.
Blood smear: A few drops of blood are used to analyze the blood under a microscope. Not proving, but indicating CLL (chronic lymphocytic leukemia), are so-called. Gumprecht umbrathat one recognizes. They are "burst" cells that burst when smeared due to the large number of cells.
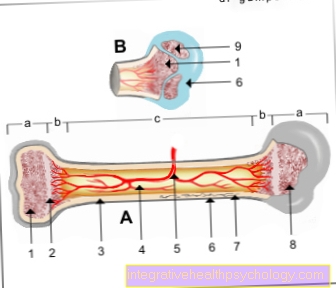
Bone marrow biopsy
The bone marrow biopsy is a removal of tissue from bone marrow. This biopsy is then also analyzed under the microscope.
Read more on the topic: Bone marrow puncture
Imaging
With the help of slice x-ray, in technical jargon called computed tomography, and ultrasound Lymph node enlargement and Organ enlargements, enlargements of the spleen and liver are typical.
therapy
Unfortunately, there is currently no cure for this disease. The therapy strategies are aimed at improving the quality of life (palliative therapy). Chemotherapy is also used here. In rare cases, irradiation of certain areas is also considered.
forecast
According to the current state of knowledge, the chronic lymphocytic leukemia is caused by drugs not curable. Only those Bone marrow transplant represents a possible, but high-risk, curative, i.e. curable, therapeutic approach.
Find out more about the topic here: Stem cell transplant
However, there have been many advances in the treatment of CLL in recent years. Often, a combination of chemotherapy and so-called antibodies succeeds in slowing the progression of the disease significantly, so that those affected long symptom-free could be.
Generally valid statements regarding life expectancy or prognosis are, as with any illness, very difficult to make.
However, various properties or characteristics of chronic lymphocytic leukemia allow conclusions to be drawn about the course of the disease.These so-called "Risk factors"Can e.g. be determined as a marker in the blood or as a feature on the leukemia cells themselves. E.g. An increased ß2-microglobulin concentration in the blood is a rather unfavorable factor and suggests a rapid progression of CLL.
The loss or exchange of individual gene segments of the leukemia cells represents a special situation. The so-called “17p deletion” and the “p53 mutation” are particularly relevant. Behind these rather bulky terms are hidden genetic changes in the chromosomes of the leukemia cells. These lead to a sometimes rapid, uncontrolled growth of cancer cells. If one of these mutations is found in a CLL patient, more aggressive drugs are used at an early stage.
In addition to the characteristics of chronic lymphocytic leukemia itself, of course also play General condition, Age and Pre-existing illness of the person concerned plays an important role.
Therefore, all possible concomitant diseases, such as High blood pressure or diabetes excluded. In addition, numerous laboratory values are analyzed, e.g. discover a possible decreased kidney or liver function.
Not to be neglected are e.g. the age, but also the physical fitness of the sick. Because the “fitter” the patients are when they are first diagnosed, the sooner they can tolerate chemotherapy and antibody therapy, which is rich in side effects.
The. Also serves as a rough guide with regard to the forecast Binet staging.
In principle, however, only the attending physician can make individual statements about the prognosis and life expectancy of those affected.
Staging
In order to ensure a uniform and generally applicable classification of chronic lymphocytic leukemia, medical professionals in Europe have relied on the so-called "Binet classification“Agreed. The CLL is used for this in 3 stages (A-C) divided. All that is needed to determine the stage is a blood and lymph node examination.
- Binet A: Less than 3 enlarged lymph node regions, increased Lymphocytes (Subspecies of white blood cells), no shortage of red blood cells and platelets.
- Binet B: More than 3 enlarged lymph node regions, increased Lymphocytes (Subspecies of white blood cells), no shortage of red blood cells and platelets.
- Binet C: Deficiency of red blood cells ("anemia", anemia), Lack of platelets (Thrombocytopenia), regardless of the number of enlarged lymph node regions.
Basically, the stages play an important role, especially when starting therapy. Patients in stage A are only treated in exceptional cases. Stage B sufferers receive therapy as soon as they experience symptoms. At stage C, one speaks of advanced chronic lymphocytic leukemia. These patients are usually always treated.
In addition, life expectancy decreases as the stage increases.
The staging according to Rai is less common, but quite applied. In contrast to the stages according to Binet, any enlargement of the liver or spleen is also included here.
Stage 0: Exclusively elevated lymphocytes (subtype of white blood cells)
Stage 1: + enlarged lymph nodes
Stage 2: + liver and / or spleen enlargement
Stage 3: + Deficiency of red blood cells ("anemia", anemia)
Stage 4: + lack of platelets