Anterior cruciate ligament tear
English: anterior cruciate ligament rupture
Synonyms in a broader sense
- ACL rupture
- Cruciate ligament lesion
- anterior knee instability anterior
- Knee instability
- anterior cruciate ligament insufficiency
- chronic anterior cruciate ligament insufficiency
- Cruciate ligament rupture
- Cruciate ligament surgery
- Cruciate ligament injury
definition
A fresh one anterior cruciate ligament tear is the complete or partial interruption of continuity (Crack) of the tape after exceeding the overstretch reserve due to external force. An old anterior cruciate ligament rupture is a permanent, mostly accident-related ligament injury.

Cause of cruciate ligament tears
Causes are often so-called "Flexion-Valgus-External Rotation Injuries". That is, the knee involuntarily bent into that X-legPosition and is turned outwards.
Typically with To ski or Soccer Such injuries happen when the lower leg is stationary.
An instability of the knee joint due to the loosening of the capsular ligament apparatus can set in.
The result is a derailment of the roll-slide mechanism and increasing degenerative (wear-related) Cartilage damage and meniscus.

I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Complaints and symptoms
An important symptom of any acute knee ligament injury is pronounced pain that occurs immediately at the moment of the trauma, then subsides immediately and returns when the load is renewed.
The rupture of the ligament structures leads to a rupture of vessels at the same time. This leads to bleeding into the knee joint (hemarthrosis). If blood is punctured during a knee joint puncture, this is always highly suspicious of a ligament injury in the knee joint.
After the acute symptoms have subsided, instability of the knee joint varies from person to person. There are complaints about instability, especially when dismounting from a meeting. Sometimes a cruciate ligament rupture is only diagnosed years after the accident.
Sometimes an anterior cruciate ligament tear can be combined with a posterior cruciate ligament tear.
Read more about the symptoms of a cruciate ligament tear under our topic: Symptoms of a cruciate ligament tear
diagnosis

Some of the patients suffer from a cruciate ligament tear strongest pain in the knee joint, this usually swells within the first few hours. The doctor will try to examine the knee with so-called stability tests.
Because of the general painfulness, this is not all that easy, as the patient tenses with his muscles.
In most cases, the examination can only take place a few days after the Torn anterior cruciate ligament can be determined, since only then is the pain from the accident reduced to such an extent that the person concerned can be examined without any defensive tension.
A normal X-ray provides information about any concurrent ones bony injuries. A bigger one Joint effusion should be punctured to relieve the cartilage and remaining soft tissues. If the effusion is bloody, it suggests a cruciate ligament tear, although this is not evidence.
With the general spread of the Magnetic resonance imaging, with which the cruciate ligaments or their remains are very clearly visible, the diagnosis can be predicted relatively reliably. In the picture above, the red arrows indicate the torn cruciate ligament (rupture of the anterior cruciate ligament).
The damage can be verified with the help of magnetic resonance imaging. The slice images show the course of the cruciate ligaments and their attachments on the upper and lower leg bones. In the event of a rupture, the fiber courses are not continuous and the localization of the tear becomes possible.
A few years ago, all patients would have to undergo surgery due to the lack of diagnostic options.
Those days are over as the Magnetic resonance imaging / MRI examination the damage that has occurred can be estimated very precisely and any necessary operations can be planned. The X-ray image is usually normal in isolated cruciate ligament ruptures. But since similar symptoms z. B. also by one Meniscal tear can be caused, it is difficult for the layperson to make a diagnosis.
Here again all the examination methods to diagnose an anterior cruciate ligament injury
Clinical diagnostics by the orthopedist:
- Assessment of knee swelling, joint effusion, range of motion and pain in motion
- Assessment of the gait pattern, leg axes
- Assessment of the femoral patellar joint (plain bearing of the kneecap)
- Assessment of knee stability and meniscus
- Muscle atrophy (thinning of the muscle relief)
- Assessment of neighboring joints
- Assessment of blood circulation, motor skills and sensitivity (feeling on the skin)
Apparative diagnostics (diagnosis using devices)
Necessary technical investigations
roentgen: Knee joint in 2 planes, patella (kneecap) tangential
Apparative investigation useful in individual cases
- X-ray: knee joint p.a. when standing in 45 degrees flexion
- Friksche image (tunnel image) to show a bony tear of the anterior cruciate ligament on the thigh bone
- Recorded recordings
- Full-leg shots under load
- Functional recordings and special projections
- Sonography = Ultrasound (e.g. for meniscus, Baker's cyst)
- Computed tomography (if there is a Tibial head fracture = Fracture of the tibial head)
- Magnetic resonance imaging (Cruciate ligaments, menisci, bone injury)
MRI is the most valuable diagnostic tool for an anterior cruciate ligament rupture, as MRI can particularly assess partial damage. An MRI for a cruciate ligament rupture helps to better assess the prognosis of the knee joint.
Please also read our topic: MRI for a cruciate ligament tear - Puncture with synovial analysis (for effusion in the knee (Water in the knee) and blood in the knee joint)
- Automated drawer inspection (no standard inspection)
classification
To the extent of a Cruciate ligament injury (Crack anterior cruciate ligament) to document is often the front drawer test carried out. The knee joint is angled 90 ° and the foot is fixed on the base. Now the examiner pulls the lower leg close to the knee joint and assesses whether the lower leg can be pulled out from the thigh.
Classification of the front drawer sign according to Debrunn
Grade I (+): slight shift 3-5 mm
Grade II (++): mean displacement 5-10 mm
Grade III (+++): pronounced displacement> 10 mm

"Front drawer" test
Figure front drawer test
Left picture with kind permission of Prof. J. Jerosch, Neuss
MRI for a cruciate ligament tear
With an experienced examiner this is diagnosis of a cruciate ligament tear usually already without imaging possible very quickly and reliably. Nevertheless, MRI has established itself as the standard method. In contrast to X-rays or CT, an MRI can namely all ligaments and soft tissues of the knee and thus basically identify existing cracks.
Partial cracks but can often only be shown very poorly in the MRI. In this respect, the MRT for making the diagnosis is less reliable than a good examination by an experienced examiner.
However, an MRI scan of the knee after an injury that can also affect the cruciate ligament is often useful.
The doctor can often use the MRI to estimate which treatment is now necessary and how quickly, if necessary, an operation should be carried out. Any injuries to other structures (meniscus, inner and outer ligament) of the knee can also often be seen well in the MRI.
This information then also has a significant influence on whether and how quickly an operation has to be carried out.
If, however, a cruciate ligament rupture is clearly evident during the examination and the circumstances of the accident do not suggest that other structures have also been damaged, an MRI is not absolutely necessary and often does not provide any new information. If an injury cannot be precisely captured and narrowed down even with an MRI, a knee examination is usually necessary.
Read more detailed information on this under our topic: MRI for a cruciate ligament tear
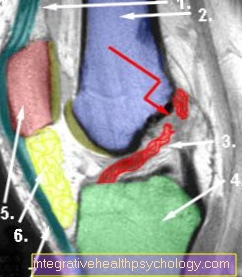
MRI image of knee with cruciate ligament tear
- Quadriceps tendon
- Thigh bone (femur)
- torn anterior cruciate ligament (red arrow shows tear site)
- Shinbone (tibia)
- Kneecap (patella)
- Hoffa's fat body
- Kneecap tendon (patellar vision)
OP at cruciate ligament tear

Surgery is usually the method of choice for a cruciate ligament tear.
Only if the posterior cruciate ligament is torn, or if there are very slight tears, can surgery be dispensed with.
However, you always run the risk that the knee will be less stable and less resilient in the long term. This is why the operation is highly recommended, especially for younger people, especially those who do sport.
However, the operation is only performed when the inflammation and swelling of the knee has sufficiently subsided. This is usually the case after about 4-6 weeks.
This waiting time is important because surgery on irritated tissue can lead to significantly poorer results. Surgery immediately after the injury is only performed in very severe cases involving bone structures.
The cruciate ligament rupture can now be operated on with minimal invasiveness, which reduces complications and accelerates healing.
The whole thing is then in the context of a knee mirror (Arthroscopy) carried out. The operation itself then consists of completely replacing the destroyed cruciate ligament with other ligament structures. Repairing the old tape will only give inadequate results. Therefore, one usually takes tape portions from adjacent tapes.
For example, the ligament of the kneecap is suitable (patella) or a thigh muscle. The portions are removed there in such a way that these bands can still fulfill their own function without any problems. The removed piece of ligament is then adjusted as precisely as possible in order to be able to take over the function of the torn cruciate ligament.
With this method, however, there can sometimes be severe pain at the removal site. This is especially the case when removing part of the patellar tendon. This type of implant usually grows in a little faster.
Ribbon portions obtained in the course of organ donation can also be used, but these have the disadvantage that rejection reactions to the exogenous material can occur. In return, the pain at the removal points of the autologous tendons is avoided.
Various systems are used to attach the band to the knee: On the one hand, simple metallic screws or fixation buttons, but also absorbable materials can be used.
The result of the operation is of course also determined by good rehabilitation.
Read more about this at: Surgery for a cruciate ligament tear
Complications of surgery
Besides the general complications an operation etc. how:
- infection
- Bleeding
- Numbness / paralysis
there are special risks associated with cruciate ligament surgery. So-called surgical complications include:
- Arthrofibrosis - a particularly feared complication. This is a partial stiffening of the knee joint after cruciate ligament surgery through scarring. The risk of arthrofibrosis is particularly high if an operation is carried out shortly after the accident.
- Cyclops syndrome - due to scarring of the cruciate ligament, which results in a stretch deficit
- Cruciate ligament plastic impingement - the cruciate ligament graft becomes wedged between the thigh rolls while stretching, preventing the knee joint from fully extending.
forecast
It has been scientifically proven that a cruciate ligament damage can cause irreparable damage to the knee joint. It is very likely that a knee joint will cause premature wear of the knee joint (osteoarthritis) after it has suffered cruciate ligament damage.
According to scientific studies, this wear and tear can be favorably influenced by the implantation of an anterior cruciate ligament, but it cannot be completely stopped.
Duration of healing
To complete healing A cruciate ligament tear should be planned for around 6-9 months. Only then is the knee usually fully resilient. Immediately after the injury knee initially for about 4-6 weeks conservative be treated.
Above all, anti-inflammatory and decongestant measures are important. Only then does the actual operation usually take place.
This is followed by the Rehabilitation phase which takes about 12 weeks to complete. In the first time after the operation, the focus is again on decongestant and anti-inflammatory measures and stabilization of the knee with a splint. Crutches must be used for a few weeks.
Then the knee is partially loaded and then adapted to the current position physical therapy. After about 6 weeks, light training on the bicycle ergometer or light walking is often possible. Less stressful sports can then be resumed after about 3-4 months. Sports that put a lot of stress on the knee, such as tennis or similar, can usually be started again after about 6-9 months, when full resilience is possible again.
Read more on this topic at: Duration of a cruciate ligament tear
Application of splints
rails are used at two points in time for cruciate ligament rupture. First, a splint can be used to cover the knee immediately after the injury stabilize and help reduce the swelling and regression of inflammation by the time of surgery.
The second important area of application is the phase immediately after the operation. During this time it is important to keep your knee closed stabilize and only allow movement within a certain framework. After all, the ligament implant attached in the operating room must first grow together with the bone in order to be really stable in the long term.
One uses rails where the Range of motion can be precisely adjusted and limited so that only a certain amount of flexion or extension is possible in the knee. So the knee can initially be in a certain position fixed become.
With this stabilization and within the framework of the movements that the splint allows, physiotherapy can already be started after a few weeks. During the healing process, the range of motion and thus the load on the knee can always be adapted to the individual healing.
This greatly reduces the risk that careless movements or overloading will damage the new ligament or delay healing after the operation.
Read more on this topic at: Cruciate ligament splint