Adnexitis
Synonyms in a broader sense
Inflammation of the uterine appendages such as the ovaries and fallopian tubes
Inflammation of the fallopian tubes, inflammation of the ovaries
English: adnexitis
Definition of adnexitis
The task of the uterine appendages is to allow the fertilizable egg to mature (Ovary) and then to transport it into the uterus, which happens via the fallopian tube.
The term adnexitis now refers to the inflammation of the ovary (Ovary) and the fallopian tube (Tuba uterina) described.

Of course, both organs, ovaries (Ovary) and fallopian tubes (tuba uterina), also be ignited separately from each other. However, such an isolated inflammation occurs extremely rarely, since the pathogens usually reach the ovary via the fallopian tubes and thus the inflammation spreads to both organs. There is a fallopian tube and an ovary both to the right and to the left of the uterus, so that the adnexitis can occur unilaterally or bilaterally.
The inflammation leads to pain in the ovaries, but these can also have many other causes and occur more frequently during pregnancy. You can read more about this topic under Ovarian Pain During Pregnancy.
The World Health Authority (WHO) coined an internationally recognized collective term that includes various chronic and acute inflammations in the pelvis. Pelvic inflammatory disease (PID) is the collective term and includes the inflammation of the fallopian tube (Salpingitis = Fallopian tube inflammation), inflammation of the ovary (Salpingoophoritis = Ovarian inflammation) and, as complications, inflammation of the peritoneum (Pelveoperitonitis = Peritonitis) and inflammation of the ligaments of the uterus (parametritis).
The Adnexitis belongs to the serious gynecological diseases. Chronic courses or long-term effects, such as Adhesions (Adhesions), one pregnancy outside the womb (Extra-lower pregnancy, as a Ectopic pregnancy) or infertility (sterility) come.
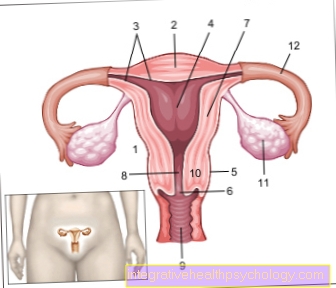
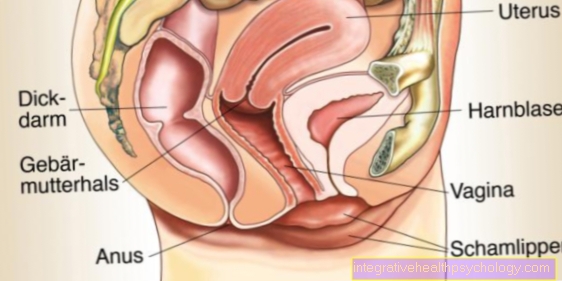
- Uterus -
uterus - Uterine tip -
Fundus uteri - Uterine lining -
Tunica mucosa - Uterine cavity -
Cavitas uteri - Peritoneum cover -
Tunica serosa - Cervix -
Ostium uteri - Uterine body -
Corpus uteri - Uterine constriction -
Isthmus uteri - Sheath - vagina
- Cervix - Cervix uteri
- Ovary - Ovary
- Fallopian tubes - Tuba uterina
You can find an overview of all Dr-Gumpert images at: medical illustrations
Epidemiology
Acute ovarian inflammation occurs in young women who are not pregnant but are sexually active.
Especially women with a high number of different sex partners, whose sexual activity began early and whose hygiene is inadequate, have an increased risk of the disease.
Every year around 11-13 new cases out of 1000 women develop the disease, with the new cases mainly being found in patients between 16 and 20 years of age.
root cause
In most cases, the cause of adnexitis is bacteria. These either get from the lower genital organs via the vagina and the uterus up to the fallopian tubes and ovaries. This path of infection is only permeable for bacteria if the normal protective barriers, such as the closed cervix, are lifted. This is for example during menstruation (Menstruation), after births or miscarriages as well as after surgery via the vagina, such as inserting the IUD or scraping the uterus. This form of ascending from below (ascendingInflammation is found almost exclusively in sexually mature and sexually active women.
Another possibility for the inflammation to spread is to descend (descending infection) of the bacteria from the abdominal organs. If a neighboring abdominal organ is inflamed, the bacteria reach the fallopian tube or ovary directly and cause adnexitis there, or the bacteria are brought to the organs via the lymphatic system and cause adnexitis as a result
Occurs after an abdominal surgery such as the removal of the appendix for appendicitis (Appendectomy) If an infection occurs in the operating area, the bacteria that have penetrated here can also lead to adnexitis.
In more than 75% of cases, the triggering bacteria are chlamydia, gonococci (Gonorrhea) and mycoplasma. Very rarely, the infection can also result from tuberculosis.
Symptoms of adnexitis
Adnexitis is inflammation of the ovaries and fallopian tubes. Adnexitis can take different forms. There are mild and symptom-free forms, but also severe courses with very strong symptoms. The most common are unilateral pelvic pain, which can also be triggered by pressure. The pain can also start suddenly and violently. Sometimes a firm structure can also be felt in the lower abdomen. If there is inflammation, an increased temperature or fever can also occur.
Read more about the topics: Inflammation of the fallopian tubes and symptoms of fallopian tube inflammation
Other common symptoms of adnexitis can be nausea, vomiting, diarrhea, but also constipation. Furthermore, due to the proximity, there may be discomfort when urinating (Dysuria) and pain during intercourse (Dyspareunia) come. Sometimes it can lead to intermenstrual bleeding, a prolonged menstrual period and purulent discharge. With severe adnexitis, the inflammation can spread to surrounding tissue and other adjacent organs. With small vibrations and movements, this can lead to severe pain in the abdominal wall. In the event of a fever in combination with severe abdominal pain, bleeding or purulent discharge, a doctor should always be consulted in order to avoid serious progress and complications. The symptoms of adnexitis can be similar in an ectopic pregnancy. There is a risk that the fallopian tube will tear, so it is important to clarify the symptoms quickly.
You can find a lot of extensive information about the symptoms under our topic: Symptoms of adnexitis
diagnosis
To suspect one Adnexitis the doctor asks about the last interventions in the area of the lower abdomen and how these were chronologically related to the menstrual period. By swabbing the vagina or the Cervix can they white blood cells (Leukocytes), which in high numbers indicate an inflammation. Usually blood is also taken to determine the signs of inflammation.
Otherwise the doctor (usually a Specialist in gynecology) trigger a pain in the cervix by touching or possibly feel the swollen fallopian tube in an advanced stage.
Pain in the ovaries In addition to adnexitis, they can also be caused by ovarian vein thrombosis and twisted stems.
With the help of Ultrasound device fluid accumulations, thickenings and enlarged ovaries can be clearly displayed and their size and extent determined.
If the diagnosis cannot yet be sufficiently confirmed by these examination methods or if the therapy has not yet been successful, a so-called Pelviscopy (endoscopic examination of the pelvic space) may be necessary under anesthesia. This examination is the only way to find a Adnexitis diagnose with certainty by looking at the focus of inflammation. In addition, a smear of the infection can be taken directly during this procedure so that the pathogen can be determined and appropriate therapy can be started. Any previous adhesions can also be loosened during this procedure.
Acute adnexitis
The acute inflammation of the fallopian tube (Tuba uterina) and / or the ovary (Ovary) is called adnexitis acuta and is characterized by sudden onset of severe pelvic pain.
This pain can be of a unilateral or bilateral nature, as the inflammation can also be unilateral or bilateral. In addition, vomiting, fever and signs of intestinal obstruction (Ileus symptoms) join.
Acute adnexitis can cause a medical emergency in the form of a so-called acute abdomen and should therefore be recognized and treated quickly. In addition, with acute adnexitis caused by certain pathogens (chlamydia), an additional inflammation of the liver (Fritz Hugh Curtis Syndrome) with right-sided upper abdominal pain and an increase in liver values.
If the acute adnexitis is not treated early and adequately, it can turn into what is known as chronic adnexitis. This causes complaints for most patients throughout their life, but they are much less pronounced and less common.
The causes of adnexitis acuta are usually ascending (ascending) Germs, which mainly enter through the vagina in sexually active women and then travel towards the fallopian tubes and ovaries. Descending (descendingInfections resulting from appendicitis (appendicitis), Peritonitis (Peritonitis) or a chronic inflammatory bowel disease such as run out of Crohn's disease.
In most cases, the pathogens are so-called chlamydia (approx.26%) or bacteria causing gonorrhea (Neisseria gonorrhea) (approx. 29%), but many other pathogens are also possible.
Acute adnexitis requires more rapid and more invasive diagnosis than would be the case with chronic adnexitis. If no cause can be found through the clinical examination in the form of a palpation examination, through the so-called speculum setting including microbiological smears and through the ultrasound examination (Sonography) can be found, the laparoscopy (laparoscopy) or the so-called pelviscopy (Pelvic reflection) with microbiological smears used earlier as a diagnostic procedure.
Once the diagnosis has been confirmed, antibiotic treatment should be started as early as possible, which should target the causative germ. In addition, surgical interventions are necessary for some patients to relieve accumulations of pus (abscesses).
In addition, pain medication can be administered to relieve pain.
As a rule, acute adnexitis requires hospitalization.
Infertility from adnexitis
Adnexitis can also develop into a chronic form, that is, into a permanent illness. Infertility can be a complication of both acute and chronic adnexitis. This is done by gluing the organ. The inflammatory fluid, the pus and the blood that arise as a result of the inflammation lead to fibrinization and thus to sticking of the organ. In this case, the ovaries and fallopian tubes.
therapy

The aim of the therapy is the fallopian tube in its complete function and thus the fertility of the woman. Therefore, immediately after taking the smear with a Antibiotic therapy began. This is done directly into the vein for 10 days, which is why an inpatient stay in the hospital is necessary. Bed rest is recommended, especially at the beginning of the illness. Sick women should drink enough fluids and have regular bowel movements and urination.
Especially in the acute phase, you can also Pain medication given in order to achieve an improvement in the general condition of the patient. In addition, the administered painkillers counteract the inflammatory process. During the acute illness phase, sexual intercourse should be avoided if possible.
Support is provided with a physical therapy began. Hourly cooling in the acute phase of the illness leads to a reduced blood flow and thus to a lower spread of the inflammation. Later, after the acute symptoms are over, the blood circulation should be increased with the help of warm, moist compresses in order to counteract adhesions.
A surgery only comes into play if other organs are affected by the acute inflammation, such as the appendix (appendix = Appendicitis) or the peritoneum (peritoneum = Bach skin inflammation). Liquids (Abscesses) can develop in the abdomen, especially between uterus and rectum (Douglas room), have accumulated. These must be punctured.
Persists after therapy glued fallopian tube and adhesions so surgery is the only way to restore fertility (Fertility), or elimination of the infertilityIn this case, the adhesions are loosened and the opening of the fallopian tube is made passable again.
When do you need antibiotics?
Most adnexitis (inflammation of the ovaries) is caused by bacteria. These can reach the fallopian tubes and ovaries via the uterus. These are most commonly chlamydia or gonococci. Since a bacterial infection can be treated most effectively with an antibiotic, an antibiotic is recommended for any adnexitis. In difficult cases it is even necessary to give the antibiotic through a vein in order to be able to fight the inflammation sufficiently. This is important so that the inflammation does not spread to the abdomen or cause sepsis (blood poisoning).
Which antibiotic is the best?
Which antibiotic is the best for treating adnexitis depends on the bacterium that caused the inflammation. Because the different antibiotics are each specialized in certain bacteria. In order to find out which bacterium it is, a sample is taken, which is examined microbiologically. Since this examination can take a few days, treatment is first carried out with a broad spectrum antibiotic. Often ciprofloxacin and metronidazole are used. These antibiotics can fight many possible bacteria. If it could be proven that the bacteria are gonococci, it is recommended to give ceftriaxone in addition. In the case of inflammation with chlamydia, azithromycin is also recommended.
Guidelines
The guidelines recommend a so-called empirical or calculated antibiotic therapy after the acceptance of Blood cultures for pathogen detection. This means the antibiotic treatment quickly (within 24-48h) must be startedwithout waiting for the result of the pathogen cultures. The antibiosis is therefore directed against the bacteriawhich are expected in the pathogen spectrum. Furthermore, it should be possible to switch to another therapy quickly after the pathogen becomes known.
This calculated antibiotic therapy should take the form of a 14-day infusion therapy Amoxicillin-Clavulanic acid and Doxycycline respectively.
Amoxicillin-clavulanic acid counteracts gram-positive and gram-negative Microorganisms which a resistance against the so-called beta lactamase. However, they are sensitive to amoxicillin-clavulanic acid and can therefore be fought by it.
Doxycycline is a subclass of the so-called antibiotic Tetracyclines and has an inhibitory effect on the growth of gram-positive, gram-negative and cell wallless bacteria (bacteriostatic effect).
If the clinical response of the Infusion therapy Oral antibiotics may be considered after a while and discharge from the hospital may be considered.
After a precise analysis of the pathogen through the blood culture, it can then switched to specific antibiotics that are precisely tailored to the pathogen to fight the pathogen even more specifically.
Differentiation between adnexitis and appendicitis
The symptoms described above can also indicate appendicitis (appendicitis). Therefore, it is difficult to differentiate between the two diseases solely on the basis of the symptoms. Appendicitis can often appear suddenly with severe pain on the right side of the lower abdomen. Fever, nausea, vomiting, and diarrhea can also occur. Adnexitis can appear both on the right and on the left.
There are several tests that can indicate appendicitis. These include two pressure points on the stomach, McBurney and Lanz. The contralateral pain of letting go can also occur with accompanying peritonitis with the adnexitis. With the help of the ultrasound, the examining doctor may be able to detect an inflamed appendix or the ovary. But the examination is not always possible or easy to carry out. If the symptoms and the examination cannot distinguish between the two diseases, a laparoscopic operation can be performed. This is a kind of mini-operation. Cameras can be used to look into the abdomen through small incisions in the skin and, if necessary, operate.
Read more about this under: Symptoms of appendicitis
prophylaxis
The use of has a proven protective effect Condoms. In addition, good hygiene and intimate hygiene are important. Prevention with hormonal contraceptives is not universally guaranteed.